Speak For Yourself’s Marcellus Wiley explained why it’s a bad idea for the NBA to paint Black Lives Matter on the court or to put the message on jerseys, and he totally nailed it. (Via RIGHT SCOOP)
Author: Papa Giorgio


Charter Schools and Their Enemies | Thomas Sowell’s New Book
Larry Elder Interviews the Great Economist and thinker, Thomas Sowell. Larry asks Sowell about Biden, the Black Lives Matter Movement, the Coronavirus Shutdown, baseball, and more… Sowell just released his new book on Charter Schools and the education system, “Charter Schools and Their Enemies” (Interview Date 7-1-2020)
The day before this show was recorded, Dr. Thomas Sowell began his 10th decade of life. Remarkably on one hand and yet completely expected on the other, he remains as engaged, analytical, and thoughtful as ever. In this interview (one of roughly a dozen or so we’ve conducted with Dr. Sowell over the years), we delve into his new book Charter Schools and Their Enemies, a sobering look at the academic success of charter schools in New York City, and the fierce battles waged by teachers unions and progressive politicians to curtail them. Dr. Sowell’s conclusion is equally thought provoking: If the opponents of charter schools succeed, the biggest losers will be poor minority children for whom a quality education is the best chance for a better life.
Dennis Prager had Thomas Sowell on his show to discuss Doc Sowell’s new book, “Charter Schools and Their Enemies”. The publisher mentions this about the book:
- The black-white educational achievement gap — so much discussed for so many years — has already been closed by black students attending New York City’s charter schools. This might be expected to be welcome news. But it has been very unwelcome news in traditional public schools whose students are transferring to charter schools. A backlash against charter schools has been led by teachers unions, politicians and others — not only in New York but across the country. If those attacks succeed, the biggest losers will be minority youngsters for whom a quality education is their biggest chance for a better life.
Carl Jackson Fills In For Dennis Prager (Larry Elder Interview)
Human Zoos (Evolution’s Dehumanizing Ethos/Racism)
This is a not-too-well-known subtitle of Charles Darwin’s work. I have an introduction to this idea entitled, “Racism and Evolutionary Thought“. Stephen Jay Gould notes the affects of Darwinism on culture:
- “Biological arguments for racism may have been common before 1850, but they have increased by orders of magnitude following the acceptance of evolutionary theory”
Stephen Jay Gould, Ontogeny and Phylogeny (Cambridge, MA: Harvard Press, 1977), 127.
Human Zoos tells the shocking story of how thousands of indigenous peoples were put on public display in America in the early decades of the twentieth century.
Above video description:
Often touted as “missing links” between man and apes, these native peoples were harassed and demeaned. Their public display was arranged with the enthusiastic support of the most elite members of the scientific community, and it was promoted uncritically by American’s leading newspapers. This award-winning documentary explores the heartbreaking story of what happened, shows how African-American ministers and other people of faith tried to push back, and reveals how some people today are still drawing on Social Darwinism in order to dehumanize others. The film also explores the tragic story of eugenics in America, the effort to breed human beings based on Darwinian principles.
Human Zoos was an official selection of the African World Documentary Film Festival and has won awards for Best Editing (Oregon Documentary Film Festival), Best in Show (Cinema WorldFest Awards) and Awards of Excellence from the Impact Docs Awards and the Hollywood Independent Documentary Awards.
Be sure to check out these other videos about social Darwinism.
Here is a small snippet from a larger audio of Carl Jackson making a point about race relations. The larger audio of Mr. Jackson filling in for Dennis Prager is here
Here Is An Older Post Originally Posted In July Of 2010

SEE MORE AT ANSWERS IN GENESIS
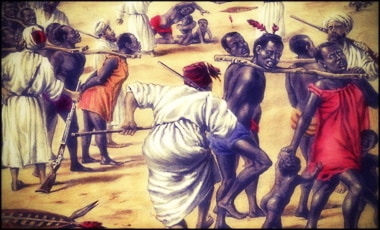
Skull-hunters killed Aborigines and legitimized this act asserting that they were doing it for science. The skulls of the hunted natives were sold to museums after some chemical reactions that would make them look old. The skulls with bullet holes were filled in with utmost attention. According to Creation Magazine published in Australia, a group of observers that came in from South Galler were shocked when they saw that dozens of women, children and men were killed by evolutionists. Forty five skulls were chosen among the killed Aborigines, the flesh of them were set aside and boiled. The best ten were packaged to be sent to England.
 |
 |
Today, thousands of skulls of Aborigines are still in the warehouse of Smithsonian Institution. Some of these skulls belong to the corpses dug from the graves where as some others are the skulls of innocent people killed to prove evolution. 
There were also African victims of the evolutionist violence. The most famous one was the pigmy Ota Benga who was taken to the world of the white men to be displayed as a transitional form. Oto Benga was caught in 1904 by a researcher Samuel Verner in Kongo then a colony of Belgium. The native whose name meant friend in his native language, was married and had two kids. Yet he was chained, put into a cage and sent by a boat to the evolutionist scientists who within the same year displayed him in the St. Louis World Fair together with other monkey species as the closest transitional form to humankind. Two years later, he was taken to Bronx Zoo in New York where he was, this time displayed as one of the ancestors of human beings together with a few chimpanzees, a gorilla called Dinah and an orangutan called Dohung. Dr. William T. Hornaday, the director of the zoo who was also a fanatical evolutionist delivered long speeches about how he was proud of having such a precious transitional form. The guests, on the other hand, treated Ota Benga as an ordinary animal. Ota Benga could not bear the treatment he received and committed suicide. (Here is a reggae song dedicated to Oto on A BITTA WORLD by BORROW SHANGO.)
From RAE:
….The many factors motivating Verner to bring Ota to the United States were complex, but he was evidently .much influenced by the theories of Charles Darwin” a theory which, as it developed, increasingly divided humankind into human contrived races (Rymer, 1992, p. 3). Darwin also believed that the blacks were an inferior race’ (Vemer, 1908a, p. 10717). Although biological racism did not begin with Darwinism, Darwin did more than any other man to popularize it among the masses. As early as 1699, English Physician Edward Tyson studied a skeleton which he believed belonged to a pygmy, concluding that this race was apes, although it was discovered that the skeleton on which this conclusion was based was actually a chimpanzee (Bradford and Blume, 1992, p. 20).
The conclusion in Vemer’s day accepted by most scientists was that after Darwin showed “that all humans descended from apes, the suspicion remained that some races had descended farther than others … [and that] some races, namely the white ones, had left the ape far behind, while other races, pygmies especially, had hardly matured at all” (Bradford and Blume, 1992, p. 20). Many scholars agreed with Sir Harry Johnson, a pygmy scholar who stated that the pygmies were “very apelike in appearance [and] their hairy skins, the length of their arms, the strength of their thickset frames, their furtive ways, all point to these people as representing man in one of his earlier forms’ (Keane 1907, p. 99). One of the most extensive early studies of the pygmies concluded that they were “queer little freaks” and
The low state of their mental development is shown by the following facts. They have no regard for time, nor have they any records or traditions of the past; no religion is known among them, nor have they any fetish rights; they do not seek to know the future by occult means… in short, they are… the closest link with the original Darwinian anthropoid ape extant” (Burrows, 1905, pp. 172, 182)….

Larry Elder On The “Hands Up, Don’t Shoot” Lie (Plus, FLASHBACKS)
Did you know: the fraudulent narrative was SO PERVASIVE that even #BlackLivesMatter was founded on this very lie.
“Hands Up. Don’t Shoot.” NEVER HAPPENED
You’ve been manipulated. Here’s the truth behind the Ferguson Lie.
- Correction: 1:33 Michael Brown was 18, not 19.
SOME FERGUSON FLASHBACKS
Michael “the Gentle Giant” Brown’s toxicology report is out… and it suggests hallucinations. This would explain well the erratic behavior some (like the Rev. Al “Not So Sharp” Sharpton) in the above clip have issue with. Here is some info from CONSERVATIVE TRIBUNE (now Western Journal):
…Eyewitness testimony has already confirmed that Brown did not have his hands up when he was shot, and the recently released county autopsy report indicates the same. In addition, forensic tests proved that Michael Brown’s blood was present on Wilson’s gun, uniform, and interior car door panel, corroborating his statement that the two struggled for control of Wilson’s gun in the car.
Now the toxicology report has been released, and it, too, puts another nail in the coffin of the liberal narrative surrounding the Brown shooting, according to The Washington Post.
“Jurors have also seen the St. Louis County autopsy report, including toxicology test results for Brown that show he had tetrahydrocannabinol, the active ingredient in marijuana, in his system,” the paper reported on Thursday.
“The Post’s sources said the levels in Brown’s body may have been high enough to trigger hallucinations,” it continued.
It’s only speculation, of course, but hallucinations could account for some of Brown’s reportedly irrational behavior that day, including his attempt to take a gun away from a trained police officer.
The race hustlers, or at least some of them, will undoubtedly portray this report as further evidence of the conspiracy to deny justice to Michael Brown, as if exonerating Wilson were a perversion of justice, rather than its necessary outcome — assuming, of course, that when all the facts are in, Wilson’s story remains credible….
Larry Elder Visited the Dennis Prager Show
Dennis Prager had Larry Elder on for his “Ultimate Issues Hour.” Larry IS an ultimate issue, so every hour of him is technically “ultimate.” I add some video both of the example Larry speaks of where Keith Ellison says George Wallace was a Republican (see LEGAL INSURRECTION for more: ). I also include a tad of the in-studio visit of Larry when he responds to a callers challenge.
Abigail Shrier’s New Book: “Irreversible Damage”
Dennis Prager had Abigail Shrier on his show to discuss her new book entitled “Irreversible Damage: The Transgender Craze Seducing Our Daughters” (see more here: ). She has been on the show previously, one appearance I truncated and is entitled, “The Trans War On Women #FairPlay“
The story regarding Amazon banning aspects of this book on their website can be found at Regnery’s website. The post is entitled,
The person’s name Dennis could not remember, I did. Walt Heyer. Walt has been on the Dennis’ Show, and I have that show which I entitled, “Sex Change Regret (Walt Heyer | Dennis Prager)“. Dennis also reads from one of Walt’s articles, here: “Child Abuse and Leftist Trans Ideals.” Walt Heyer’s site, SEX CHANGE REGRET.
Cul-De-Sac Commandos (St. Louise Couple): Tucker | Hodge Twins

(From the comments) Wow. So the “Private property” sign didn’t stop the crooks? But GUNS did????? Who would have thought!!!!
Tucker Carlson takes on Indiana Sen. Mike Braun on ‘Tucker Carlson Tonight.’

Rev. Stephen Schumacher Provide a History Lesson on King Louis IX
MODERN GHANA notes a bit of the history referenced in the video:
- Gadhafi’s unbridled urge in modern times to enlarge Arabia inside Africa, is a continuation of the Arab war against Africans and the Arabization of African lands that started in the 7th century CE. Arabs have since settled on one-third of Africa, pushing continuously southwards towards the Atlantic Ocean. Arabs’ racial war against Black Africa started with their occupation and colonization of Egypt between 637 and 642 CE, decimating the Coptic or Black population. Between 642 and 670 CE, more Arab invaders poured into Africa and occupied areas known today as Tunisa, Libya, Algeria and Morocco, where they physically eliminated most of the native (Berber) inhabitants. The Berbers that escaped death ran westwards and southwards towards the Sahara.
It is interesting that as Rev. Stephen Schumacher (a priest with the St. Louis Archdiocese) is attempting to provide a history lesson on King Louis IX, h is being shouted at with Afrocentrist history (taught by black racist cults like The Nation of Islam and the Five Percenters).
THE DAILY WIRE has a good post on this:
….Rev. Schumacher, in a video which can be viewed below, attempted to inform protesters about King Louis IX.
“St. Louis was a man who had authority thrust upon him, he didn’t do anything to earn it. You’re right, he didn’t do anything to earn it,” started the priest. “What did he do with that authority? Do you know what he did? Go down to the St. Louis Cathedral, and you’ll see some of the history that St. Louis did.”
One of the protesters shouted, “Eventually we’re taking that, too, though,” referencing the cathedral.
“St. Louis was a man who willed to use his kingship to do good for his people,” Rev. Schumacher said, triggering angered shouts from protesters.
“He died in Tunisia,” one of the protesters shouted, drawing an alleged connection to Africans.
“St. Louis had nothing to do with Africans, okay,” the Catholic leader responded to protesters.
“Do you know who lived in Tunisia in the 1100s?” he posed, “Arabs. … and the Arabs had killed all the Africans in Tunisia in the 700s.”
“In the 700s, Arab Muslims conquered the Holy Land,” Rev. Schumacher continued, “Christians did not fight back against that. … the Crusades happened beginning in 1095, after the Turks conquered the Holy Land.”
During the same intense face-off, some protesters marked the statue with chalk, calling for its destruction, reported Currier.
[….]
“The history of the statue of St. Louis, the King is one founded in piety and reverence before God, and for non-believers, respect for one’s neighbor,” the statement said. “The reforms that St. Louis implemented in French government focused on impartial justice, protecting the rights of his subjects, steep penalties for royal officials abusing power, and a series of initiatives to help the poor.”
“King Louis IX’s renowned work in charity helped elevate him to Sainthood,” the St. Louis Archdiocese continued. “His daily suppers were shared with numerous beggars, whom he invited to the royal table. On many evenings, he would not let them leave before he washed their feet. He personally paid to feed more than 100 poor Parisians every day. His care for the sick was equally moving; St. Louis frequently ministered to lepers. He also created a number of hospitals, including one for the blind and another for ex-prostitutes.”….
Some Anti-Semitism Via Twitter
Take note my handle is Deplorable Pony Soldier, and I provide some context for the retards.
I will post the main Tweet, followed by mine and the Jewish conspiracy people:





What The Left Won’t Tell You About The History Of Slavery
Virginia Senator Tim Kaine isn’t a particularly stupid man. Wrong, perhaps, and often so – but not stupid. But he must really think you are. (More at MRCTV-blog)

MAGA Hulk | “Charlotte Scott” Discuss Emancipation (+David Barton)
Absolute INSANITY. Statues depicting Murderous Racists stay up… but the Left wants to DESTROY the men that EMANCIPATED the slaves? Stephen Davis has a message for all the Liberals trying to ERASE His History.
- Historical reenactor Marcia Cole is opposed to tearing down Lincoln statue in DC
- She portrays Charlotte Scott, who donated the first $5 for statue in 1865
- Parks service says the statue was solely funded by freed former slaves
- Now, Black Lives Matter protesters vow to tear the statue of Lincoln down
- They say the depiction of the former slave below Lincoln is demeaning
BONUS
(Via my page: U.S. RACIAL HISTORY)
David Barton 3-Part (Video) Series
The One-Size-Fits-all Approach To The WuFlu Authoritarian, Inefficient
Dr. Scott Atlas is the Robert Wesson Senior Fellow at the Hoover Institution, an accomplished physician, and a scholar of public health. For several weeks, Dr. Atlas has been making the case in print and in other media that we as a society have overreacted in imposing draconian restrictions on movement, gatherings, schools, sports, and other activities. He is not a COVID-19 denier—he believes the virus is a real threat and should be managed as such. But, as Dr. Atlas argues, there are some age groups and activities that are subject to very low risk. The one-size-fits-all approach we are currently using is overly authoritarian, inefficient, and not based in science. Dr. Atlas’s prescription includes more protection for people in nursing homes, two weeks of strict self-isolation for those with mild symptoms, and most importantly, the opening of all K–12 schools. The latter recommendation is vital for restarting and maintaining the economy so that parents are not housebound trying to work and educate their children. Dr. Atlas is also adamant that an economic shutdown, and all of the attendant issues that go along with it, is a terrible solution—the cure is worse than the disease. Finally, Dr. Atlas reveals some steps he’s taken in his own life to try to get things back to normal.