(An older two posts somewhat combined with a new Tweet added by Robby Starbuck)
Larry Elder goes through the lies of the media and Democrats saying Trump called the Coronavirus a hoax. Democrat politicians and the Media (and some #NeverTrumpers) continue to spread this untruth, like they did the Charlottesville Lie and the lie that Trump made fun of a man’s handicap. The other DOUBLE-STANDARD by the media is that they themselves called the Coronavirus the Chinese Virus or Wuhan Virus themselves. When the “Bad Orange Man” used it they switched gears and said it was racist.
Here are some posts I think are worthy to compliment the audio:
Fact Check: Did Trump Call Coronavirus a ‘Hoax’? (DAILY SIGNAL)
Media Claim Trump Called Coronavirus A ‘Hoax.’ But Video Shows That’s Not What Trump Said at All (THE BLAZE)
Woke Media Calls Term ‘Wuhan Virus’ Racist After Using Term ‘Wuhan Virus’ (THE FEDERALIST)
[WATCH] 35 Times the Media Said ‘Wuhan Coronavirus’ or ‘Chinese Coronavirus’ (PJ-MEDIA)
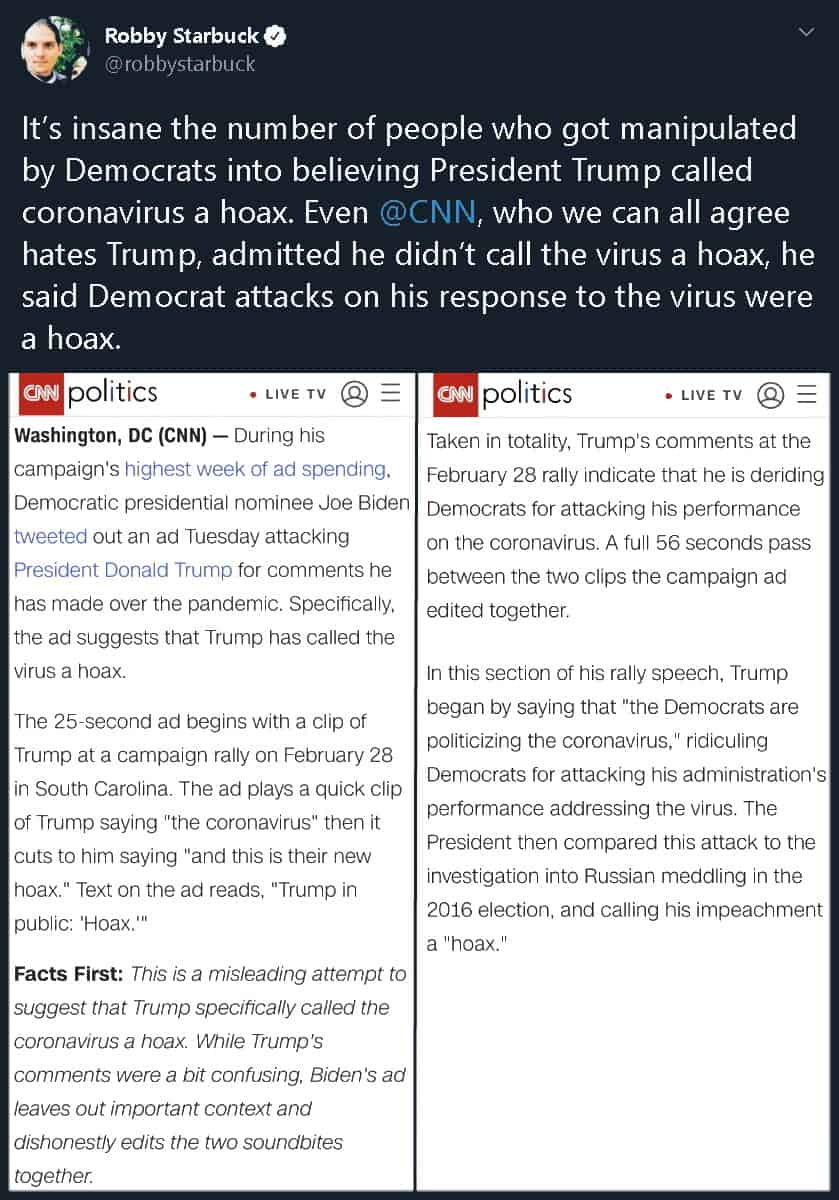
Click on the graphic to open it, then click on the graphic to enlarge it. This comes via Robby Starbuck:
Democrats and the media (and #NeverTrumpers) try to say that the Trump administration refused and slowed test kits for the Wuhan Virus (COVID-19). This just is not the case, as the interview Larry Elder excerpts from between Dr. Anthony Fauci and Hugh Hewitt (YOUTUBE) shows clearly.
BONUS
The media and Democrats push false Trump coronavirus narrative.
AMERICAN THINKERruns some good Tweets by Steve Guest (You can find the entire Twitter thread HERE):
MUZZLED?! CUT FUNDING?!
Earlier this week, Michael Bloomberg and Joe Biden were called out by the AP for lying about President Trump cutting funding to the CDC and NIH.
The facts from the Associated Press: Financing has increased to the CDC and the NIH.https://t.co/DZ7549XNL0
When the AP fact-checks Democrats… you know its bad. More from an earlier AMERICAN THINKER article:
…To set the stage, here are a few indisputable facts:
On January 31, 2020, as China confirmed that 259 people had died and there were about 100 cases reported outside of China, President Trump ordered that the U.S. would prevent foreign nationals who had recently visited China from entering the country. He also ordered quarantined American travelers who posed a high risk.
President Trump held a press conference during which (1) he was surrounded by government scientists who explained what was going on (2) he appointed Vice President Pence, a competent, experienced administrator, to be the White House point person on coronavirus efforts.
Democrats also announced that henceforth they would call coronavirus “TrumpVirus” because Trump had appointed Pence to oversee the administrative end of dealing with coronavirus and because Trump said there was no need for panic.
Nancy Pelosi complained that Trump had waited too long to act, even though when she spoke not a single American had died.
Elizabeth Warren said that she would end the “racist” border wall by taking all wall funds and putting them into coronavirus research (never mind that, since time immemorial, sealing borders has been one of the prime ways in which governments have been able to protect their citizens from epidemic disease).
Trump stated during the rally in South Carolina that the Democrats’ unceasing and dishonest attacks against him for his handling of the coronavirus risk were their latest hoax.
The media reported that Trump had declared that coronavirus itself was a hoax, one of the most blatantly dishonest bits of reporting ever to come from the media.
Leftists are actively hoping that coronavirus causes so much economic disruption that it will hurt Trump politically – never mind that it will also hurt ordinary Americans….
Senator and “Doctor of the Year,” Scott Jensen, MD, was interviewed on MSM about the new and unorthodox way he was instructed to fill out death certificates by the CDC, as well as comparing Coronavirus and the seasonal flu, a statement already made by Tony Fauci and other officials. In a shocking turn of events, his medical license is now under review by the state of Minnesota. Jensen has publicly stated he has “no regrets,” and talks to Del about how he’s even more inspired to speak out.
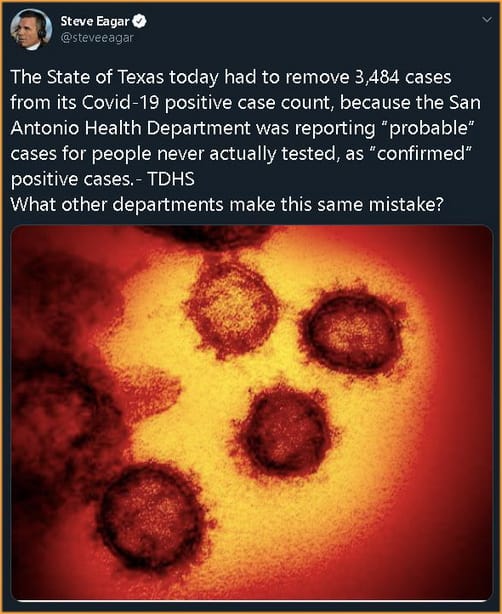
The change in cases comes as questions have been raised across the country about coronavirus testing, most notably in Florida. An investigation in the state determined that the test positivity rate reported by officials was inaccurate and that the number of positive tests was much lower than reported.
In May, coronavirus task force member Dr. Deborah Birx suggested that the actual number of coronavirus cases could be inflated by as much as 25%, while others have argued that cases have been undercounted.
Questions about the number of coronavirus cases have also been raised in Colorado, Pennsylvania, and New Jersey over claims that suspected coronavirus patients are dying from causes other than the virus.
CHICKS ON THE RIGHT note that the real question “becomes how accurate can the antigen test be?” Continuing, this is hinted that it does not fair well for other than strep.
The question We see that an antigen test for strep is accurate but the rapid test for the flu is not. NPR reported, “Researchers do not expect it to be as accurate as the PCR diagnostic test, but it is possible the antigen tests could be used to screen patients for infection. Dr. Jordan Laser, a lab director at Northwell Health, notes antigen testing is used for rapid strep tests, which are reliable, and rapid flu tests, which are not.”
We haven’t even created an accurate test for the flu. The flu that has been around all of my life, and we cannot figure out how to create an accurate rapid test, but we are supposed to believe an antigen test for a brand new virus is accurate?
This is serious. We are being lied to by the Democrat cities where they have labs that conveniently are showing 100% positive rates, but after audits are more around the 9% rate and some labs are even lower than that. They use these high numbers to justify shutting down businesses and schools and locking everyone at home.
SENT POSITIVES WITH NO TEST
One of the managers at Von’s told me today his wife’s sister or his sister (I forget what he said) had made an appointment to get tested for Covid. He said she cancelled, but a few days later received a notice she was positive. Here is another confirmation of such shenanigans:
And as states are going over death certificates, they are dropping by at least 25% in deaths by Covid-19. And some independent groups are helping “catch” the inflated number, like Pennsylvania’s “Wolf administration was caught this week adding up to 269 fake deaths to the state totals on Tuesday” (CITADELPOLITICS). Or this short example (PJ-MEDIA)
On Thursday, the Washington State Department of Health (DOH) confirmed a report by the Freedom Foundation that they have included those who tested positive for COVID-19 but died of other causes, including gunshot injuries, in their coronavirus death totals. This calls into serious question the state’s calculations of residents who have actually died of the CCP pandemic.
Last week, after it was reported that, like Washington, Colorado was counting deaths of all COVID-19 positive persons regardless of cause (which had resulted in the inclusion of deaths from alcohol poisoning), the Colorado Department of Health and Environment began to differentiate between deaths “among people with COVID-19” and “deaths due to COVID-19.”
Just one more of the many examples I could share is the New York Times getting 40% wrong of their “died from Covid-19 under 30-years old” front page news story. Mmmm, no, they didn’t die of Covid. As states figure this out, the inflated counts (like when Colorado did this — fell by 25%: lots more on this below).
[….]
On Thursday, the Washington State Department of Health (DOH) confirmed a report by the Freedom Foundation that they have included those who tested positive for COVID-19 but died of other causes, including gunshot injuries, in their coronavirus death totals. This calls into serious question the state’s calculations of residents who have actually died of the CCP pandemic.
First up, Dr. Birx setting the stage for this with how deaths are coded:
Another example comes from Dr. Ngozi, Director of public health Illinois. She explains how ALL deaths are counted as Covid-19 even if the patient was diagnosed to have die from another disease:
Adapted from the above video description is important (via 4 TIMES A YEAR)
“Should “COVID-19” be reported on the death certificate only with a confirmed test? COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death.” (CDC): “Deborah Birx, a physician who’s leading the White House’s coronavirus task force, said Alabama’s strategy conflicts with CDC’s approach to tallying Covid-19-realted deaths. “[W]e’ve taken a very liberal approach to mortality,” she said. “[I]f someone dies with Covid-19, we are counting that as a Covid-19 death.” (ADVISORY)
As many have pointed out, there is a big difference between dying WITH the virus and FROM the virus.
Note Dr. Birx’s similar wording to what Italy was doing:
“‘We’ve taken a very liberal approach to mortality….” “The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus.”
Italy, unlike the CDC, corrected its error:
“The age of our patients in hospitals is substantially older – the median is 67, while in China it was 46,” Prof Ricciardi says. “So essentially the age distribution of our patients is squeezed to an older age and this is substantial in increasing the lethality.”
A study in JAMA this week found that almost 40 per cent of infections and 87 per cent of deaths in the country have been in patients over 70 years old.
[….]
But Prof Ricciardi added that Italy’s death rate may also appear high because of how doctors record fatalities.
“The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus.
“On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus, while 88 per cent of patients who have died have at least one pre-morbidity – many had two or three,” he says.
[….]
If further testing finds more asymptomatic cases spreading undetected, the mortality rate will drop.
1) The shocking inflation of COVID-19 death numbers: From day one, we were warned that states are ascribing every single death of anyone who happens to test positive for the coronavirus — even if they are asymptomatic — to the virus rather than the clear cause of death. Now, thanks to a lawsuit in Colorado, the state was forced to revise its death count down by 23 % over the weekend — from 1,150 to 878. The state is now publishing numbers of deaths “with” COVID-19 separate from deaths “from” COVID-19. As I reported on Thursday, county officials started accusing the state’s department of health of reclassifying deaths of those who tested positive for the virus but died of things like alcohol poisoning as COVID-19 deaths just to insidiously inflate the numbers. This revision in Colorado is a bombshell story that, of course, will remain unknown to most Americans. Every state needs to do this, and if they did, we would find an across-the-board drop in numbers by at least 25%, the same %age by which Dr. Birx reportedly believes the count is being inflated, according to the Washington Post. For example, in Minnesota, state officials are now admitting that every single person who dies in a nursing home after testing positive is now deemed to have died from the virus, never mind the fact that 25% of all natural deaths in a given week occur in nursing homes and that most cases of COVID-19 are asymptomatic, which means more often than not, they died exclusively of other causes.
TO WIT… Dennis Prager’s guest is Dr. Joel Hay, who is a professor in the department of Pharmaceutical Economics and Policy at the University of Southern California. Both give examples of cancer deaths being coded Covid:
And my third evidence to support my contention a nurse is filmed commenting on the percentages of deaths at NYC hospital. In my posts point #2 (the video still up amazingly) notes that every death cert in NYC-hospital is coded as Rona. In fact, 99% of deaths from that hospital were coded Rona during a period — AN IMPOSSIBLE statistic (my site)
….In New York City, around 12,000 people have supposedly died from COVID-19 at the time of this writing. That’s 22% of all alleged U.S. deaths.
Around 7,000 of the NYC deaths attributed to COVID-19 have been thoroughly investigated to determine if there was another serious life-threatening illness present
Take a deep breath if doing so hasn’t been outlawed where you live.
99.2% of those 7,000 New Yorkers who supposedly died from the virus had another antecedent life-threatening illness. For all intents and purposes, that’s all of them.
How is it even remotely possible that 7,000 NYC deaths attributed to COVID-19 were investigated and virtually every single one of them found to have involved at least one other life-threatening illness if the virus is in and of itself deadly?
Most strains of coronavirus that affect humans are common cold viruses.
In light of the apparent almost universal prevalence of at least one other deadly disease among the alleged NYC deceased…
And in light of all the factors massively inflating the bogus death tally we’re being fed every day…
What reason do we have to believe COVID-19 is actually killing anyone?
No one knows how many Americans have really died of COVID-19….
However, we are starting to find out that “pure” deaths caused by Covid-19 exclusivelt is low (DAILY WIRE):
On Tuesday, San Diego county Supervisor Jim Desmond said after digging into the data that he believes only six of the county’s 194 coronavirus-identified deaths are “pure” coronavirus deaths, meaning they died from the virus, not merely with the virus.
Desmond was seemingly ruling out deaths from individuals with preexisting conditions.
“We’ve unfortunately had six pure, solely coronavirus deaths — six out of 3.3 million people,” Desmond said on a podcast, Armstrong & Getty Extra Large Interviews, according to San Diego Tribune. “I mean, what number are we trying to get to with those odds. I mean, it’s incredible. We want to be safe, and we can do it, but unfortunately, it’s more about control than getting the economy going again and keeping people safe.”
Public Health Officer Dr. Wilma Wooten suggested Wednesday during a press briefing that Desmond was being callous, noting that their liberal identification of COVID-19 deaths is uniform with coding nationwide.
“Their life is no less valuable than someone’s life who does not have underlying medical conditions,” Wooten said. “This is not just San Diego. This is how this is done throughout the entire nation in terms of identifying who has died of COVID-19.”…
AUDIO BELOW the hospitalizations excerpts/updates:
…Lindsey Rosales, a spokeswoman for the Texas Department of State Health Services, confirmed to Just the News this week that the state is categorizing every inpatient in the state with a positive COVID-19 test as a COVID-19 hospitalization. … (JUST THE NEWS)
AMERICAN THINKERnotes the following, “We are told new cases are rising by double-digit percentages, including: “The number of people hospitalized with coronavirus.” Hospitalized with or from coronavirus? Is this really a surge or simply fear-mongering fake news?” Continuing they quote a Texas area hospital CEO:
….A Texas hospital CEO lets the fake news cat out of the bag.
Health officials in Texas are logging every single COVID-19-positive hospital patient in the state as a COVID-19 hospitalization, even if the patients themselves are admitted seeking treatment for something other than the coronavirus.
Most hospitals require a COVID test before elective surgery. This means that patients coming to the hospital for a non-COVID reason are tested for COVID, and if positive are being counted as a “COVID hospitalization.” If a patient goes to the hospital for a new hip or cataract surgery, and happens to test positive for COVID, they are counted as a COVID hospitalization.
Just like inflated death counts, there is a big difference between dying or being hospitalized due to coronavirus or with coronavirus. George Floyd tested positive for COVID but no one is attributing his death in Minneapolis to COVID. Yet that is how hospitalizations are being counted, leading to this so-called surge in cases.
This surge hit the news about two weeks ago, after the BLM protests and riots peaked and agitators were starting to be arrested. Is this the latest chapter in the ongoing saga to beat on Trump and interfere in the upcoming presidential election?…..
AUDIO
Larry O’Connor spoke with Dr. Scott Atlas, the Robert Wesson Senior Fellow at the Hoover Institution of Stanford University, about the latest surrounding the country reopening following the coronavirus.
Dr. Scott Atlas, former chief of neuroradiology at Stanford University Medical Center and a senior fellow at Stanford’s Hoover Institution, offered a potential explanation about why COVID hospitalizations are rising among younger people in Texas.
Appearing on Monday night’s “The Story with Martha MacCallum,” Atlas said that, since everyone who gets hospitalized for any reason is getting tested for COVID-19, the people making up the inflated statistics could actually be “hospitalized for something else” but “classified as COVID-19 hospitalizations.”
“What is your thought on that, do you think that 25% of the cases are being hospitalized are people 20-29, does that seem unusual?” MacCallum asked.
“No,” Atlas said. “I think that’s counter to any other data point we have. We have a state that has detailed evidence, Florida. We see that although there is a huge rise in cases, they are almost all overwhelmingly healthy young people. They are not being hospitalized. They are not dying. The deaths are going down per day. The hospitalizations are going down per day. It’s just not likely.”
“I think that what is happening in Texas, I know that this is true, they are testing every person that gets hospitalized for Covid-19,” Atlas continued. “We know that the vast majority of people with COVID-19 who are young, particularly, are asymptomatic or minimally symptomatic. I question if those people who are positive for COVID-19 and being hospitalized for something else are classified as COVID-19 hospitalizations. That’s a big difference.”
Atlas went on to explain that younger people getting the infection is actually a good thing because it leads to herd immunity over the long term…….
To date, residents in 250 long-term care facilities in Washington State have tested positive for COVID-19. More than 500 deaths, some 60% of all pandemic deaths in the state, have occurred in such institutions, according to the Seattle Times. Parallel figures are 41% in Ohio and 66% in Arizona.
No one lives forever. Jesus recognized the ugliness of death. But the terrible thing about this disease is how it tears families apart, isolating the elderly just when they need comfort. Instead of a warm hand and eyes of loved ones as they face that “final frontier,” with final words of encouragement in their ears (or on their lips), millions struggle for breath surrounded by rows of beds with others coughing, while medical personnel — harassed, tired, and sometimes fearful strangers — rush in dressed like aliens in space suits.
I mentioned to a friend that I guarantee this kid has been influenced by the Nation of Islam or the 5%’ers when I saw this on the 21st — from my Facebook:
This is one of the most maddening things I have seen in a while! CAUTION, violence:
This is a nursing home. Please someone explain why this is happening and unreported. pic.twitter.com/Dzs8QYykIv
…Jaydon Hayden is reportedly from Westland, Michigan and beat elderly white nursing home patients for sport.
There are three videos right now on Bitchute showing the man beating white people.
The man is filming himself beating the seniors in their beds until they are bleeding….
Well, I am vindicated in my assumprion. But, before getting to it, there is an update to this story that answers “what was this guy doing at a nursing homw to begin with”? GATEWAY PUNDIT fills us in:
Jaydon Hayden, reportedly from Westland, Michigan filmed himself beating elderly white nursing home patients for sport.
The man filmed himself beating the the elderly man, later identified as a 75-year-old veteran, in his bed until he was bleeding.
[….]
On Friday FOX 2 Detroit in Michigan spoke with the father of the Jaydon Hayden after his arrest.
The father said his son is not vicious, but that he just has mental health issues.
And the father then said this,
“He said his son called 911 and was taken to a mental health facility in Ann Arbor. Last Wednesday, he was diagnosed with COVID-19 and said he was supposed to be taken to another facility to be quarantined.
The father added, “It should’ve never happened because he should’ve never been put in that environment.”
Did you catch that?
Authorities — following the orders of Governor Gretchen Whitmer — moved the young man to a nursing home to recover from COVID-19.
They moved 20-year-old Jaydon Hayden to the nursing home just last week.
According to his father, Jaydon Hayden was moved to the nursing home because he had COVID-19.
This tells us that Governor Whitmer is STILL sending COVID-19 patients to NURSING HOMES.
And Democrat Governor Whitmer is STILL sending coronavirus patients to nursing homes!
WOW! After all we know about the elderly and The Wu Flu, a Democrat Governor is still sending Covid positive patients to nursing homes. Unbelievable!
Well, this whole horrible issue is now a confirmation in some way of my noting this as a racist cult issue. But this also proves the father’s point as well, he has some mental issues… needless to say the mental and Coronavirus issues would negate placing him in a nursing home.
Prager reads from a WALL STREET JOURNAL article about how the doctors were wrong by a factor of 50 regarding predicted deaths of the sailors on board from the WuFlu.
Here are some key points from a reproduced article not behind a “pay-wall” (APK METRO):
….The medical group’s warning, the small print of which haven’t beforehand been reported, indicated that there was a “excessive chance” that as much as 1% of the roughly 4,800-member crew—or “50 or extra” sailors—might die, and that a whole bunch of sailors would fall unwell. The restricted medical services on Guam, the place the ship by then had docked to dump sailors sickened with Covid-19, would quickly be overwhelmed, the docs wrote.
“We is not going to stand by whereas our fellow sailors proceed to be uncovered to this deadly virus,” the memo stated. “The time has come for aggressive measures to be taken and we’re asking to your assist.”
[….]
Roughly 1,200 crew members grew to become sick whereas the ship was docked in Guam and one of many provider’s crew, Chief Petty Officer Charles Robert Thacker Jr., 41, died of the virus on April 13.
[….]
The views expressed within the one-page medical memo, summing up an air of urgency aboard the provider on the onset of the outbreak, partially prompted Capt. Crozier to write down his personal memo, despatched to senior Navy leaders about the identical time. Capt. Crozier’s memo grew to become the topic of reports stories, resulting in his elimination. The warning that 50 sailors might die was reported by the New York Times in April….
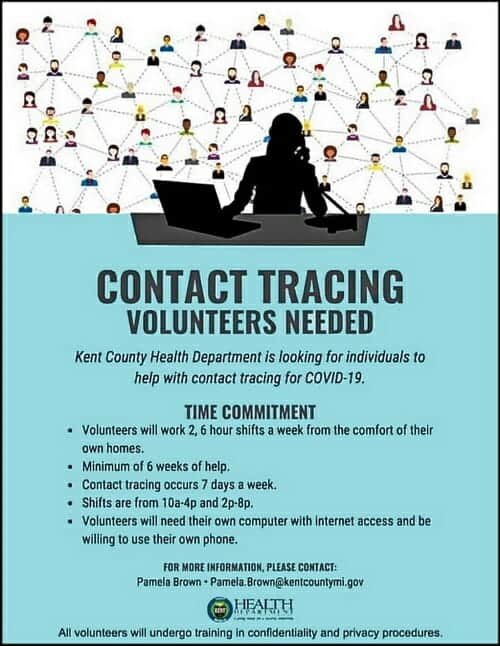
Authorities have found a new excuse to delay reopening America: The need for hundreds of thousands of so-called ‘contact tracers.’
Bill Gates suggests mass surveillance of Americans to combat coronavirus pandemic.
The Covid-19 pandemic is likely to have a long-lasting impact not just on the world economy and the global population but also on the way we use our gadgets. To keep up with the changes brought by the pandemic, tech giant Apple has released iOS 13.5 with Face ID enhancements, Exposure Notification API and more.
iOS 13.5 speeds up access to the passcode field on devices with Face ID when the user is wearing a mask. Several users who wear masks, were facing difficulty unlocking their handset with Face ID. The Face ID would reject the login attempt multiple times and then the option to enter passcode will appear, causing significant delay.
With iOS 13.5 update, the iPhone will detect when the user is wearing a face mask and the passcode field will now be automatically presented after swiping up from the bottom screen.
The feature is only available on devices with Face ID, that is, iPhone X, iPhone XS, iPhone XS Max, iPhone XR, iPhone 11, iPhone 11 Pro, and iPhone 11 Pro Max. This also works when the user is authenticating with the App Store, Apple Books, Apple Pay, iTunes and other apps which support signing in with Face ID.
iOS 13.5 also comes with an Exposure Notification API, which supports Covid-19 contact tracing apps from public health authorities.The exposure notifications, for the uninitiated, are alerts that users will receive on their phones if they have been exposed to someone who has tested positive for or is highly likely to test positive for Covid-19….
(emphasis added)
The original post (OP) on this second strain was a graphic. I will link to the Kent County (Michigan site through it. Here is my FB description of the following: “A person named B.M. wrote on a friends Facebook wall the following regarding “contact tracing.” (The original post had to do with hiring government employees to trace citizens with Covid.)”
[A reader of JP’snoted] Actually, contact tracing sounds like a legitimate work of government. Rather than quarantining the healthy, quarantine the sick and monitor those exposed to the disease.
JP responded:
Sorry in advance for the novel! Heh, I started thinking of other interesting things to add and just decided to run with it.
Contact tracing might work for illnesses that don’t spread very easily (it probably would have exterminated HIV, according to what I’ve read; I’m no expert but it seems reasonable), but for upper respiratory stuff like colds and flus (and the Wu Flu), it’s pretty much doomed, especially with up to 10% of the whole country already having the it.
The original point of the lockdowns (which don’t seem to have worked; lockdown and non-lockdown countries and states have almost identical statistics) was to slow the spread to prevent hospitals from being overwhelmed. It wasn’t to stop spread, since even the CDC admits that after about 1% of people are infected with a contagious disease, you can’t really close the door on it anymore. Contact tracing is a relatively invasive way of closing the door on a virus, so I don’t think it will work here**.
The data points to a much less lethal bug, though. Stanford’s meta analysis of all of the large-scale antibody testing shows an IFR (Infection Fatality Rate) between 7 times less than the seasonal flu and 2.8 times more. It’s probably in the middle, making it slightly less lethal than regular seasonal flus. And since we know it has been in the US at least since January (probably since December or earlier), the R? (Basic Reproduction Number or Rate) is also much lower than people originally thought. So it spreads like the flu and is as deadly as the flu.
The main difference seems to be the 24/7 media terrorizing of citizens, the complete ignorance most of us (that’s me, too) had in the real pneumonia/influenza deaths each year, and the downright evil policy of many Democrat governors of sending the sick to recover (while contagious) at nursing homes, boosting the deaths by up to 50%.
Sorry for the novel!! Reading every little bit about this thing has become an unfortunate hobby of mine. I’m of the mind now that the best strategy is to fight the fear instead of the virus and to get back to normal in virtually every way. If this is anything like it’s older brother SARS, it will die out in the next couple of months. But if not, keeping everyone from immunity just means extending the risk.
**I think contact tracing may -appear- to work because I think we are naturally bottoming out cases. Same, in my mind, for other measures.
One final bit: I’ve followed lots of different predictions to see who might get things most accurately to see what they did differently. This guy’s been right on (it’s been almost scary) using SARS as a comparison instead of the Spanish Flu (since this bug is SARS 2). This is a really good visual of the whole thing:
(Click to enlarge)
ALSO, a short bit from Bruce Carrol:
“If you are waiting for a “cure” for COVID-19, you’ll never leave your home again.
Even the flu vaccine (not vaccine, flu shot. There is a vaccine for the Polio, not HIV or SARS) results in 60-80,000 deaths every season.
We have to stop the fearmongering and start learning to live with a new virus in a string of new viruses that have emerged for tens of thousands of years.
Boomers and Millennials aren’t that special of a species.”
— Bruce Carroll (Co-founder of the gay Republican group GOProu, and founder of GAYPATRIOT)
More than half of U.S. deaths are from nursing homes — THE GUARDIAN:
Yale professor describes as ‘staggering’ research that reveals more than half of all deaths in 14 US states from elderly care facilities
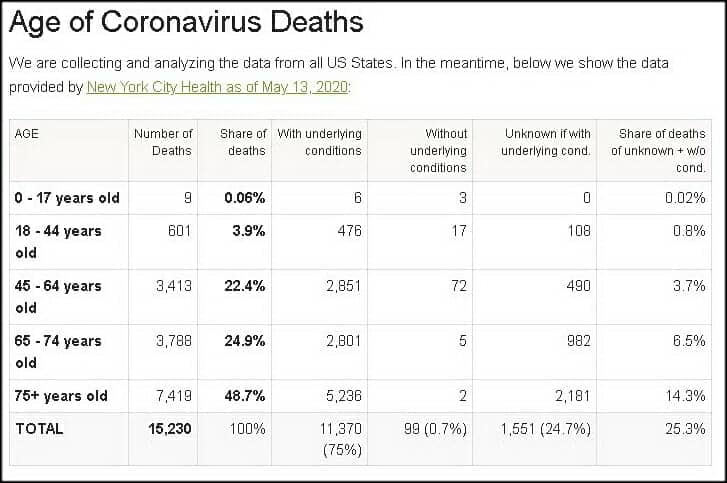
The average age group who dies from “The Rona” is found here in the latest from WORLD O’METER:
Not only that, but the co-morbidities (just as in flu deaths) are high and in multiples. Some examples:
Of the 22,332 people who died in hospital in England between 31 March and 12 May, 5,873 (26%) suffered from either type 1 or type 2 diabetes, NHS England figures reveal. That was the most common illness found in an analysis of what existing conditions patients had. The other commonest comorbidities were dementia (18%), serious breathing problems (15%) and chronic kidney disease (14%). One in ten (10%) suffered from ischaemic heart disease. (GUARDIAN)
A new study published April 22 in the Journal of the American Medical Association characterizes the symptoms, comorbidities, and clinical outcomes of 5,700 patients hospitalized because of COVID-19 in the New York area. The authors found that 94 percent of the patients had a chronic health problem, and 88 percent had two or more. The three most prevalent conditions were hypertension (56.6 percent), obesity (41.7 percent), and diabetes (33.8 percent). (THE SCIENTIST)
Now, many of these deaths were preventable, but for some reason many of the hardest hit states had a tragic policy of sending elderly patients back to nursing homes to recover. Many of the blue states, where most of the deaths have occurred:
If you live in New Jersey, you are 13 times more likely to die from COVID-19 than if you live in Florida. The Garden State’s death rate per million is 895.2, according to the RealClearPolitics coronavirus tracker, compared to only 65.1 deaths per million for Florida. This disparity can’t be written off to demography or testing. Florida has a huge elderly population, and it has conducted twice as many tests as New Jersey. (AMERICAN SPECTATOR)
I have a slew of articles regarding this deadly choice by Andrew Cuomo on my site (FULLY reproduced here):
MAY I ALSO NOTE that I believe the deaths from The Rona are a bit overstated, while Dr. Birx noted that the CDC may be inflating the death toll by 25%, I provide a couple other examples to support my claim. First up, Dr. Birx setting the stage for this with how deaths are coded:
Another example comes from Dr. Ngozi, Director of public health Illinois. She explains how ALL deaths are counted as Covid-19 even if the patient was diagnosed to have die from another disease:
1) The shocking inflation of COVID-19 death numbers: From day one, we were warned that states are ascribing every single death of anyone who happens to test positive for the coronavirus — even if they are asymptomatic — to the virus rather than the clear cause of death. Now, thanks to a lawsuit in Colorado, the state was forced to revise its death count down by 23 % over the weekend — from 1,150 to 878. The state is now publishing numbers of deaths “with” COVID-19 separate from deaths “from” COVID-19. As I reported on Thursday, county officials started accusing the state’s department of health of reclassifying deaths of those who tested positive for the virus but died of things like alcohol poisoning as COVID-19 deaths just to insidiously inflate the numbers. This revision in Colorado is a bombshell story that, of course, will remain unknown to most Americans. Every state needs to do this, and if they did, we would find an across-the-board drop in numbers by at least 25%, the same %age by which Dr. Birx reportedly believes the count is being inflated, according to the Washington Post. For example, in Minnesota, state officials are now admitting that every single person who dies in a nursing home after testing positive is now deemed to have died from the virus, never mind the fact that 25% of all natural deaths in a given week occur in nursing homes and that most cases of COVID-19 are asymptomatic, which means more often than not, they died exclusively of other causes.
TO WIT… Dennis Prager’s guest is Dr. Joel Hay, who is a professor in the department of Pharmaceutical Economics and Policy at the University of Southern California. Both give examples of cancer deaths being coded Covid:
And my third evidence to support my contention a nurse is filmed commenting on the percentages of deaths at NYC hospital. In my posts point #2 (the video still up amazingly) notes that every death cert in NYC-hospital is coded as Rona. In fact, 99% of deaths from that hospital were coded Rona during a period — AN IMPOSSIBLE statistic (https://tinyurl.com/y9awsuor — my site)
….In New York City, around 12,000 people have supposedly died from COVID-19 at the time of this writing. That’s 22% of all alleged U.S. deaths.
Around 7,000 of the NYC deaths attributed to COVID-19 have been thoroughly investigated to determine if there was another serious life-threatening illness present
Take a deep breath if doing so hasn’t been outlawed where you live.
99.2% of those 7,000 New Yorkers who supposedly died from the virus had another antecedent life-threatening illness. For all intents and purposes, that’s all of them.
How is it even remotely possible that 7,000 NYC deaths attributed to COVID-19 were investigated and virtually every single one of them found to have involved at least one other life-threatening illness if the virus is in and of itself deadly?
Most strains of coronavirus that affect humans are common cold viruses.
In light of the apparent almost universal prevalence of at least one other deadly disease among the alleged NYC deceased…
And in light of all the factors massively inflating the bogus death tally we’re being fed every day…
What reason do we have to believe COVID-19 is actually killing anyone?
No one knows how many Americans have really died of COVID-19….
However, we are starting to find out that “pure” deaths caused by Covid-19 exclusivelt is low (DAILY WIRE):
On Tuesday, San Diego county Supervisor Jim Desmond said after digging into the data that he believes only six of the county’s 194 coronavirus-identified deaths are “pure” coronavirus deaths, meaning they died from the virus, not merely with the virus.
Desmond was seemingly ruling out deaths from individuals with preexisting conditions.
“We’ve unfortunately had six pure, solely coronavirus deaths — six out of 3.3 million people,” Desmond said on a podcast, Armstrong & Getty Extra Large Interviews, according to San Diego Tribune. “I mean, what number are we trying to get to with those odds. I mean, it’s incredible. We want to be safe, and we can do it, but unfortunately, it’s more about control than getting the economy going again and keeping people safe.”
Public Health Officer Dr. Wilma Wooten suggested Wednesday during a press briefing that Desmond was being callous, noting that their liberal identification of COVID-19 deaths is uniform with coding nationwide.
“Their life is no less valuable than someone’s life who does not have underlying medical conditions,” Wooten said. “This is not just San Diego. This is how this is done throughout the entire nation in terms of identifying who has died of COVID-19.”…
Also note that all the anti-body tests are showing a larger infected population than previously considered. REASON.COM previously noted the Stanford study that between “48,000 and 81,000 residents of Santa Clara County, California are likely to have already been infected by the coronavirus that causes COVID-19.” Stanford University has revised the numbers to better fit the assumption (via MERCURY NEWS):
…In a revised analysis of a startling study published last month, they now estimate that 2.8% of Santa Clara residents were previously infected by the virus but didn’t know it.
That implies that the county had up to 54,000 infections — many more than the 1,000 confirmed cases in the county at the time.
“This suggests that the large majority of the population does not have antibodies and may be susceptible to the virus,” concludes the research paper, published in the online report medRxiv….
MY COMMENTS FROM MY FACEBOOK ABOUT THE ABOVE
So, Stanford settled on a number in early April… when there were 1,000 CONFIRMED cases were known in Santa Clara, there were 54,000 infected. To REALLY understand the percentages you would have to follow those 1,000 KNOWN cases from that time and compare the 55,000 cases to those deaths. (BTW, Stanford took the lower path on stats; so there could be a larger number.) Here is part of the article… but know that with the flu shot, there are more deaths by the flu than The Rona, without a “Rona shot.”
UPDATE (trying to figure out deaths per infections): Okay, let us apply the 98% survive who are known to have it and are hospitalized stat I have heard for some time. So 2% of the 1,000 is 20. 20 deaths from that early April figure of 55,000. Right? Gives you… 0.036%
UPDATES!
A friend on FACEBOOK has been a light in the war-torn field of The Rona (Wu Flu) battle of infection rates. Here are two posts of his [combined with a response to a friendly comment from one of his peeps] followed by some recent articles (links to papers will be in graphics):
Here’s a new meta-study from Stanford of all of the antibody testing that’s happened.
This puts the Wu Flu anywhere between 7x LESS deadly than the flu and 2.8x MORE deadly than the flu (making it a little worse than a bad flu season like 2018). And that’s assuming that this doesn’t follow SARS 1 and just disappear.
The data behind this is really solid, and the author is well-respected. Unlike those stupid models we were using, this is really real data.
We don’t do contact tracing, social distancing, mask-wearing, or lockdowns for the seasonal flu, and this looks like a watered down seasonal flu that got 100000000x more media attention and governors sending sick people to nursing homes to boost up the death rate.
The original post (OP) on this second strain was a graphic. I will link to the Kent County (Michigan site through it. Here is my FB description of the following: “A person named B.M. wrote on a friends Facebook wall the following regarding “contact tracing.” (The original post had to do with hiring government employees to trace citizens with Covid.)”
[A reader of JP’snoted] Actually, contact tracing sounds like a legitimate work of government. Rather than quarantining the healthy, quarantine the sick and monitor those exposed to the disease.
JP responded:
Sorry in advance for the novel! Heh, I started thinking of other interesting things to add and just decided to run with it.
Contact tracing might work for illnesses that don’t spread very easily (it probably would have exterminated HIV, according to what I’ve read; I’m no expert but it seems reasonable), but for upper respiratory stuff like colds and flus (and the Wu Flu), it’s pretty much doomed, especially with up to 10% of the whole country already having the it.
The original point of the lockdowns (which don’t seem to have worked; lockdown and non-lockdown countries and states have almost identical statistics) was to slow the spread to prevent hospitals from being overwhelmed. It wasn’t to stop spread, since even the CDC admits that after about 1% of people are infected with a contagious disease, you can’t really close the door on it anymore. Contact tracing is a relatively invasive way of closing the door on a virus, so I don’t think it will work here**.
The data points to a much less lethal bug, though. Stanford’s meta analysis of all of the large-scale antibody testing shows an IFR (Infection Fatality Rate) between 7 times less than the seasonal flu and 2.8 times more. It’s probably in the middle, making it slightly less lethal than regular seasonal flus. And since we know it has been in the US at least since January (probably since December or earlier), the R? (Basic Reproduction Number or Rate) is also much lower than people originally thought. So it spreads like the flu and is as deadly as the flu.
The main difference seems to be the 24/7 media terrorizing of citizens, the complete ignorance most of us (that’s me, too) had in the real pneumonia/influenza deaths each year, and the downright evil policy of many Democrat governors of sending the sick to recover (while contagious) at nursing homes, boosting the deaths by up to 50%.
Sorry for the novel!! Reading every little bit about this thing has become an unfortunate hobby of mine. I’m of the mind now that the best strategy is to fight the fear instead of the virus and to get back to normal in virtually every way. If this is anything like it’s older brother SARS, it will die out in the next couple of months. But if not, keeping everyone from immunity just means extending the risk.
**I think contact tracing may -appear- to work because I think we are naturally bottoming out cases. Same, in my mind, for other measures.
One final bit: I’ve followed lots of different predictions to see who might get things most accurately to see what they did differently. This guy’s been right on (it’s been almost scary) using SARS as a comparison instead of the Spanish Flu (since this bug is SARS 2). This is a really good visual of the whole thing:
(Click to enlarge)
ALSO, a short bit from Bruce Carrol:
“If you are waiting for a “cure” for COVID-19, you’ll never leave your home again.
Even the flu vaccine (not vaccine, flu shot. There is a vaccine for the Polio, not HIV or SARS) results in 60-80,000 deaths every season.
We have to stop the fearmongering and start learning to live with a new virus in a string of new viruses that have emerged for tens of thousands of years.
Boomers and Millennials aren’t that special of a species.”
— Bruce Carroll (Co-founder of the gay Republican group GOProu, and founder of GAYPATRIOT)
One of the great unknowns of the COVID-19 crisis is just how deadly the disease is. Much of the panic dates from the moment, in early March, when the World Health Organization (WHO) published a mortality rate of 3.2 percent — which turned out to be a crude ‘case fatality rate’ dividing the number of deaths by the number of recorded cases, ignoring the large number of cases which are asymptomatic or otherwise go unrecorded.
The Imperial College modeling, which has been so influential on the UK government, assumed an infection fatality rate (IFR) of 0.9 percent. This was used to compute the infamous prediction that 250,000 Britons would die unless the government abandoned its mitigation strategy and adopted instead a policy of suppressing the virus through lockdown. Imperial later revised its estimate of the IFR down to 0.66 percent — although the March 16 paper which predicted 250,000 deaths was not updated.
In the past few weeks, a slew of serological studies estimating the prevalence of infection in the general population has become available. This has allowed Prof John Ioannidis of Stanford University to work out the IFR in 12 different locations.
They range between 0.02 percent and 0.5 percent — although Ioannidis has corrected those raw figures to take account of demographic balance and come up with estimates between 0.02 percent and 0.4 percent. The lowest estimates came from Kobe, Japan, found to have an IFR of 0.02 percent and Oise in northern France, with an IFR of 0.04 percent. The highest were in Geneva (a raw figure of 0.5 percent) and Gangelt in Germany (0.28 percent).
The usual caveats apply: most studies to detect the prevalence of the SARS-CoV-2 virus in the general population remain unpublished, and have not yet been peer-reviewed. Some are likely to be unrepresentative of the general population. The Oise study, in particular, was based on students, teachers and parents in a single high school which was known to be a hotspot on COVID-19 infection. At the other end of the table, Geneva has a relatively high age profile, which is likely to skew its death rate upwards.
But it is noticeable how all these estimates for IFR are markedly lower than the figures thrown about a couple of months ago, when it was widely asserted that COVID-19 was a whole magnitude worse than flu. Seasonal influenza is often quoted as having an IFR of 0.1 to 0.2 percent. The Stanford study suggests that COVID-19 might not, after all, be more deadly than flu — although, as Ioannidis notes, the profile is very different: seasonal flu has a higher IFR in developing countries, where vaccination is rare, while COVID-19 has a higher death rate in the developed world, thanks in part of more elderly populations.
The Stanford study, however, does not include the largest antibody study to date: that involving a randomized sample of 70,000 Spanish residents, whose preliminary results were published by the Carlos III Institute of Health two weeks ago. That suggested that five percent of the Spanish population had been infected with the virus. With 27,000 deaths in the country, that would convert to an IFR of 1.1 percent.
This backs up of course some excellent article by Daniel Horowitz:
A CLEARER PICTURE has a great post about this as well, I suggest if you like what you see you check out that blog weekly.
…For one thing, Dr. Fauci and Dr. Birx have both explicitly stated that anyone dying WITH the virus is counted as dying FROM it. Since 4/5 of COVID-19 infections are mild and 1/2 appear to show no symptoms at all, the official U.S. death tally is bound to include many in which it played little or no role.
The CDC has made matters much worse by insisting that doctors list COVID-19 on death certificates without a positive test confirming its presence and even absent any medical justification at all. A willingness to “assume” it was a factor is all that’s officially required. And hospitals now reap enormous financial rewards for making the assumption.
(Click To Enlarge)
Those in charge couldn’t have possibly shown less interest in determining the real number of Americans who would still be alive if not for having contracted COVID-19. It’s unlikely that ours is the only country in which the data has been turned into garbage by a perfect storm of inflating factors. As hard as it may be to accept, the odds are pretty much nil that we’ll ever know how deadly the virus we were made to spend months obsessively fearing really was.
Even on the inflated numbers we’re getting, however, it isn’t anywhere near 10 times deadlier than the flu; as Dr. Fauci claimed on March 11, while ginning up support for his novel public health strategy of extinguishing our rights and wrecking the economy. But, of course, a few weeks later, we learned that even Fauci didn’t believe a word of the lie he so effectively used to terrorize a nation of over 300 million people into suicidal obedience.
Though perhaps you haven’t heard. You see, on March 26, Dr. Fauci shared his true opinion with his peers in the pages of the prestigious New England Journal of Medicine:
The overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%).
Dr. Anthony Fauci, March 26, 2020 New England Journal of Medicine
In case you’re wondering, the parenthetical remark is his, not mine. Moreover, when Sharyl Attkisson contacted the journal about the strange discrepancy between what Fauci was scaring the public with and the substantially less alarming take his learned colleagues heard, she discovered his article had been submitted “many weeks ago.”….
Rush Limbaugh on Friday’s show (May 15th) took a call that led him to an important response that places like New York that survive off of their Manhattan business district may lose [permanently] large corporations renting out the office space and paying the high cost of taxes that fund the city and are a large portion of taxes. The people that live and work in the tri-state areas that are also connected to making New York City run (BLUE COLLAR: maintenance, janitorial, tech, etc.) as well as all the business professionals (WHITE COLLAR: administrators, human resources, lawyers, etc.). Not only that, but the new laws and enforcements like these seen in this pandemic may be a cost for companies moving their offices to other states.
Manhattan Faces a Reckoning if Working From Home Becomes the Norm: Even after the crisis eases, companies may let workers stay home. That would affect an entire ecosystem, from transit to restaurants to shops. Not to mention the tax base
Here are a couple other note-worthy articles:
Manhattan New Rentals Plunge 71% as Coronavirus Freezes Market (NBC – NECN)
Would Gov. Cuomo Rather Have No Businesses in New York Than Businesses That Employ Fewer People? His proposed law would require that corporations return bailout funds if they don’t rehire the same number of employees (REASON)
‘If It Saves Just One Life’: Layoffs Start to Hit Media and Suddenly They Notice the Problem (RED STATE)
100,000 Businesses Have Permanently Collapsed Under Pandemic Lockdowns (THE FEDERALIST)
If we sacrifice to Big Government our freedom, our money, our jobs, our future, and our dignity, in return Big Government will abolish death. That premise is the basis of the lockdown strategy for dealing with the Wuhan coronavirus.
The premise is a lie. Death is part of life. Elderly people with preexisting conditions dying from viruses is not something that will stop no matter how big the government.
Dave Morrison has some interesting thoughts on the futility of the devastating lockdown, which is a far larger problem than the virus itself:
In addition to record unemployment numbers, experts now predict that a “wave” of small business bankruptcies is on the horizon — and it could leave the United States with 40% fewer small businesses.
The New York Times reports that the United States Chamber of Commerce estimates “more than 40 percent of the nation’s 30 million small businesses could close permanently in the next six months” — a statistic entirely attributable to the coronavirus pandemic and ensuing lockdowns.
The economic consequences of such a mass business failure could last for “generations,” the NYT reports.
“Commercial bankruptcies in the first quarter of 2020 ticked up 4 percent from a year earlier, according to data from the American Bankruptcy Institute,” according to the NYT. “But many of those filings were made before the pandemic, when the economy was healthy. Right now, some owners are waiting to find out if they will receive federal stimulus aid before deciding whether to file for bankruptcy protection.”
Restaurants and retail services are, of course, the most vulnerable, but family-owned enterprises, like heating and cooling operations and plumbing companies, and even health-care services, particularly small dental and pediatric practices, are in severe danger. The Small Business Restructuring Act, which took effect in February, could help some small businesses stay above water, but many are struggling to keep people on the payroll, to compete with unemployment insurance, and to handle mounting debt.
Of course, large companies — and, in particular, large retail outlets — are not immune to the economic effects of coronavirus. Brands like Neiman Marcus, J. Crew, JC Penney, Macy’s, Gap, GNC, and David’s Bridal are all staring down the possibility that their stores may not reopen once coronavirus lockdowns are lifted, according to USA Today. CNBC says that at least 150 companies, from airline conglomerates to healthcare providers, have warned investors to expect major earnings hits.
The bad economic news keeps piling. In addition to closures, a jobs report, due out from the Department of Labor on Thursday, “will almost certainly show that the coronavirus pandemic inflicted the largest one-month blow to the U.S. labor market on record,” per the Wall Street Journal……
Do fast shutdowns work to combat the unfold of Covid-19? Joe Malchow, Yinon Weiss and I needed to search out out. We got down to quantify what number of deaths have been brought on by delayed shutdown orders on a state-by-state foundation.
To normalize for an unambiguous comparability of deaths between states on the midpoint of an epidemic, we counted deaths per million inhabitants for a set 21-day interval, measured from when the dying charge first hit 1 per million—e.g.,‒three deaths in Iowa or 19 in New York state. A state’s “days to shutdown” was the time after a state crossed the 1 per million threshold till it ordered companies shut down.
We ran a easy one-variable correlation of deaths per million and days to shutdown, which ranged from minus-10 days (some states shut down earlier than any signal of Covid-19) to 35 days for South Dakota, one in every of seven states with restricted or no shutdown. The correlation coefficient was 5.5%—so low that the engineers I used to make use of would have summarized it as “no correlation” and moved on to search out the true reason behind the issue. (The trendline sloped downward—states that delayed extra tended to have decrease dying charges—however that’s additionally a meaningless consequence because of the low correlation coefficient.)
No conclusions could be drawn concerning the states that sheltered rapidly, as a result of their dying charges ran the total gamut, from 20 per million in Oregon to 360 in New York. This vast variation implies that different variables—like inhabitants density or subway use—have been extra necessary. Our correlation coefficient for per-capita dying charges vs. the inhabitants density was 44%. That implies New York Metropolis may need benefited from its shutdown—however blindly copying New York’s insurance policies in locations with low Covid-19 dying charges, akin to my native Wisconsin, doesn’t make sense.
(CLICK TO ENLARGE)
Sweden is preventing coronavirus with common sense tips which can be a lot much less economically damaging than the lockdowns in most U.S. states. Since individuals over 65 account for about 80% of Covid-19 deaths, Sweden requested solely seniors to shelter in place slightly than shutting down the remainder of the nation; and since Sweden had no pediatric deaths, it didn’t shut down elementary and center colleges. Sweden’s containment measures are much less onerous than America’s, so it will possibly preserve them in place longer to forestall Covid-19 from recurring. Sweden didn’t shut down shops, eating places and most companies, however did shut down the Volvo automotive plant, which has since reopened, whereas the Tesla plant in Fremont, Calif., was shuttered by police and stays closed.
How did the Swedes do? They suffered 80 deaths per million 21 days after crossing the 1 per million threshold stage. With 10 million individuals, Sweden’s dying charge‒and not using a shutdown and big unemployment‒is decrease than that of the seven hardest-hit U.S. states—Massachusetts, Rhode Island, Louisiana, Connecticut, Michigan, New Jersey and New York—all of which, besides Louisiana, shut down in three days or much less. Regardless of tales about excessive dying charges, Sweden’s is in the midst of the pack in Europe, akin to France; higher than Italy, Spain and the U.Okay.; and worse than Finland, Denmark and Norway. Older individuals in care properties accounted for half of Sweden’s deaths.
We must always cheer for Sweden to succeed, not ghoulishly bash them. They could show that many features of the U.S. shutdown have been errors—ineffective however economically devastating—and level the way in which to correcting them.
Mr. Rodgers was founding CEO of Cypress Semiconductor Corp.