….According to a CDC review of 113 studies, COVID-19 is only contagious ranging from two to three days before symptom onset to eight days after.
“That’s why the CDC recommends that people be exempted from any sort of PCR surveillance testing for 90 days after a positive test,” Gigi Gronvall, PhD, senior scholar at the Center for Health Security at the Johns Hopkins Bloomberg School of Public Health, told Verywell. Gronvall works with the center’s COVID-19 Testing Toolkit. “I expect that that this guidance is probably going to change at some point with more information, but some people continue to test positive by PCR even after they’re clearly no longer infectious. For whatever reason, there is still viral genetic material hanging out in their nose.”
Rapid tests are less sensitive, but a person will probably still test positive for six or seven days after they are no longer having symptoms, Gronvall said.
I disagree with Bill Maher on the “Climate Change ‘denial'” thingy (now “Climate Emergency” — see Patrick Moore’s book “Fake Invisible Catastrophes and Threats of Doom” for instance), but this is a worthy rant of note:
Study: Majority Of Americans Grossly Overestimated COVID-19 Hospitalization Rates (THE FEDERALIST)
I also think he is partially correct on the weight issue. There are other factors as well. For instance,
Almost 60 percent of patients, 47 percent of women and 67 percent of men, were vitamin D deficient on admission (a level of 25(OH)D <20 ng/mL). The deficiency was worst in men with the most severe pneumonia. The correlation of vitamin D deficiency with death, with an odds ratio of 3.87, was independent of age or comorbidities.
The report, published in the American Journal of Clinical Pathology, notes that studies involving hundreds to thousands of individuals in the U.S. and Israel showed an association between prior vitamin D deficiency and the possibility of a positive PCR test. Studies involving tens to hundreds of patients in Iran, Germany, Israel, Spain, China, and the UK reported correlations between low vitamin D levels and intensive care unit (ICU) admission, ventilator dependency, and death.
Beside its role in calcium metabolism, 1,25-dihydroxyvitamin D stimulates defenses against pathogen invasion of the respiratory tract and inhibits the destructive “cytokine storm.” Deficiency has been associated with more frequent viral respiratory infections and asthma attacks.
More than a billion people worldwide are deficient, Dr. DeSmet writes.
About 20 minutes of daily sun exposure to a large area of skin, between 11:00 a.m. and 2:00 p.m., is needed to make enough vitamin D. Darker-skinned individuals need more. As the weather cools, vitamin D levels will be dropping—note that “flu season” happens when vitamin D levels are depleted after winter sun deprivation. Adults may need 4,000 to 5,000 IU of vitamin D3 supplements daily.
More than 90 percent of nursing home patients are reportedly vitamin D deficient. This might help explain why they account for around half of COVID deaths though they represent less than 1 percent of the population. Does supplementation help? In a French nursing home, COVID survival in patients who had recently received an oral bolus of 80,000 IU of vitamin D3 was 82 percent, compared with 44 percent in those who had not (adjusted hazard ratio, 0.11, P = 0.003—see figure below)….
One studyTrusted Source found that, overall, about 42% of people in the United States were deficient in vitamin D. The figure rose to 82% among Black people and 70% among Hispanic people. (MEDICAL NEWS TODAY)
Researchers at Boston University School of Medicine (BUSM) analyzed data from 235 people who were admitted to the hospital with Covid-19. They found that patients older than 40 years old were 51.5 percent less likely to die from the infection if they had a sufficient level of Vitamin D, which they define as being at least 30 ng/mL. (FORBES)
I posted this on my Facebook and got immediate reactions… here is the video:
While I mentioned in my post “I LOVE this woman!,” it is a store policy… and I myself would wear it. However, here is the comment and my responses, followed by a newer audio upload — while Jim G. responded (not effectively to include here), my only purpose here is to post some resources for people to track down:
MY RESPONSES
Here’s Dr. Fauci in January:
Click to go to NATURE
I DIDN’T POST THIS ONE… BUT THE READER HERE CAN USE IT:
Why can’t America’s healthcare system be more like Canada’s? Here’s a better question: why would you want it to be? French-Canadian entrepreneur Alain Lambert has first-hand experience with both Canada’s and America’s healthcare systems, and he offers some cautionary tales. Canadian-style healthcare might not be as good for your health as you think.
This next short video is by filmmaker Stuart Browning, who provides a cautionary lesson about a politicized health care system where politicians and bureaucrats determine medical priorities. See more at Dr. Brownings (dated) SITE.
Stossel: Government-run health care may mean waiting in line for care. (ABC News blocked this from playing on my site, so click through to watch it at YouTube):
Claude Castonguay, the father of the Canadian Health Care system, and a model adopted by the NHS in Britain, has said his model is failing:
Just yesterday, I wrote about how unpopular the British healthcare system has become. Today comes news that the man largely responsible for Canada’s conversion to a single-payer health care system has admitted the system’s failure:
“Back in the 1960s, (Claude) Castonguay chaired a Canadian government committee studying health reform and recommended that his home province of Quebec — then the largest and most affluent in the country — adopt government-administered health care, covering all citizens through tax levies.
The government followed his advice, leading to his modern-day moniker: “the father of Quebec medicare.” Even this title seems modest; Castonguay’s work triggered a domino effect across the country, until eventually his ideas were implemented from coast to coast.”
Four decades later, as the chairman of a government committee reviewing Quebec health care this year, Castonguay concluded that the system is in “crisis.”
“We thought we could resolve the system’s problems by rationing services or injecting massive amounts of new money into it,” says Castonguay. But now he prescribes a radical overhaul: “We are proposing to give a greater role to the private sector so that people can exercise freedom of choice.”
As more and more nations throughout the world seek to infuse more private, market-based solutions into their government-controlled healthcare systems, for some reason lefties in this country want to make the same mistake that countries like Canada made decades ago…
One person eventually wrote a book about their experience, noting in a CITY JOURNAL article:
…I was once a believer in socialized medicine. I don’t want to overstate my case: growing up in Canada, I didn’t spend much time contemplating the nuances of health economics. I wanted to get into medical school—my mind brimmed with statistics on MCAT scores and admissions rates, not health spending. But as a Canadian, I had soaked up three things from my environment: a love of ice hockey; an ability to convert Celsius into Fahrenheit in my head; and the belief that government-run health care was truly compassionate. What I knew about American health care was unappealing: high expenses and lots of uninsured people. When HillaryCare shook Washington, I remember thinking that the Clintonistas were right.
My health-care prejudices crumbled not in the classroom but on the way to one. On a subzero Winnipeg morning in 1997, I cut across the hospital emergency room to shave a few minutes off my frigid commute. Swinging open the door, I stepped into a nightmare: the ER overflowed with elderly people on stretchers, waiting for admission. Some, it turned out, had waited five days. The air stank with sweat and urine. Right then, I began to reconsider everything that I thought I knew about Canadian health care. I soon discovered that the problems went well beyond overcrowded ERs. Patients had to wait for practically any diagnostic test or procedure, such as the man with persistent pain from a hernia operation whom we referred to a pain clinic—with a three-year wait list; or the woman needing a sleep study to diagnose what seemed like sleep apnea, who faced a two-year delay; or the woman with breast cancer who needed to wait four months for radiation therapy, when the standard of care was four weeks….
One of David Gratzer’s books opened my eyes to what was going on up in Canada and gave me ammunition to respond to silly liberal emotive arguments. The book is “Code Blue: Reviving Canada’s Health Care System.” But, many people believe the Michael Moore’s of the World:
Some More Videos
Obamacare, Trumpcare, Ryancare, Berniecare. Doesn’t matter what you call it, when you hand over control of healthcare to the Government through a single-payer, universal system: it sucks. Allow me, someone who grew up with socialized medicine in Montreal, Canada, explain why.
Government-controlled health care in Canada is “great unless you need it.” Ralph Weber, a Canadian medical refugee, explains why he and his family got the medical care they needed, not in Canada, but in the United States. Is Canada style waiting lists and rationing headed south, with the passage of ObamaCare?
This is another video I wish to save and it comes from CATO Institute. See more here “featuring Stuart Browning with a critique of SiCKO“. I believe the longer video is gone — sad. See more at Dr. Brownings (dated) site.
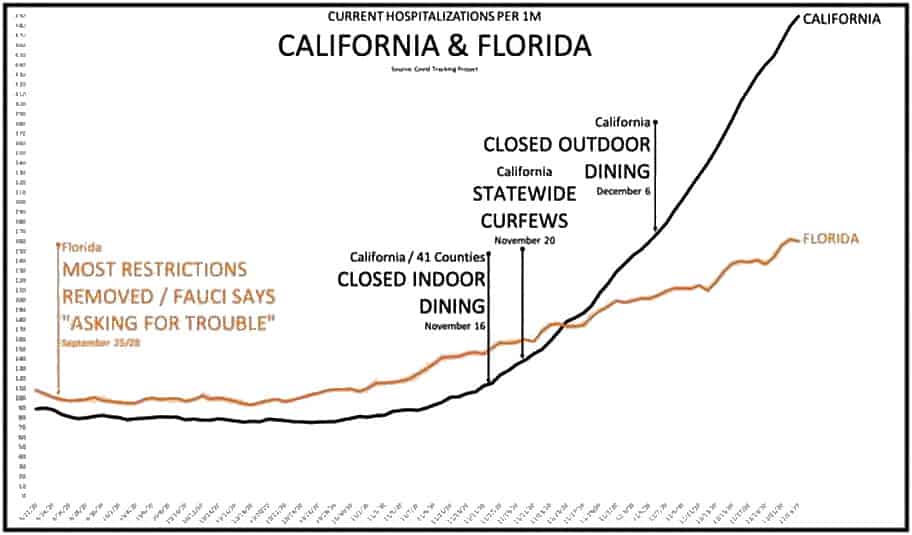
AUDIO BELOW the hospitalizations excerpts/updates:
…Lindsey Rosales, a spokeswoman for the Texas Department of State Health Services, confirmed to Just the News this week that the state is categorizing every inpatient in the state with a positive COVID-19 test as a COVID-19 hospitalization. … (JUST THE NEWS)
AMERICAN THINKERnotes the following, “We are told new cases are rising by double-digit percentages, including: “The number of people hospitalized with coronavirus.” Hospitalized with or from coronavirus? Is this really a surge or simply fear-mongering fake news?” Continuing they quote a Texas area hospital CEO:
….A Texas hospital CEO lets the fake news cat out of the bag.
Health officials in Texas are logging every single COVID-19-positive hospital patient in the state as a COVID-19 hospitalization, even if the patients themselves are admitted seeking treatment for something other than the coronavirus.
Most hospitals require a COVID test before elective surgery. This means that patients coming to the hospital for a non-COVID reason are tested for COVID, and if positive are being counted as a “COVID hospitalization.” If a patient goes to the hospital for a new hip or cataract surgery, and happens to test positive for COVID, they are counted as a COVID hospitalization.
Just like inflated death counts, there is a big difference between dying or being hospitalized due to coronavirus or with coronavirus. George Floyd tested positive for COVID but no one is attributing his death in Minneapolis to COVID. Yet that is how hospitalizations are being counted, leading to this so-called surge in cases.
This surge hit the news about two weeks ago, after the BLM protests and riots peaked and agitators were starting to be arrested. Is this the latest chapter in the ongoing saga to beat on Trump and interfere in the upcoming presidential election?…..
AUDIO
Larry O’Connor spoke with Dr. Scott Atlas, the Robert Wesson Senior Fellow at the Hoover Institution of Stanford University, about the latest surrounding the country reopening following the coronavirus.
Dr. Scott Atlas, former chief of neuroradiology at Stanford University Medical Center and a senior fellow at Stanford’s Hoover Institution, offered a potential explanation about why COVID hospitalizations are rising among younger people in Texas.
Appearing on Monday night’s “The Story with Martha MacCallum,” Atlas said that, since everyone who gets hospitalized for any reason is getting tested for COVID-19, the people making up the inflated statistics could actually be “hospitalized for something else” but “classified as COVID-19 hospitalizations.”
“What is your thought on that, do you think that 25% of the cases are being hospitalized are people 20-29, does that seem unusual?” MacCallum asked.
“No,” Atlas said. “I think that’s counter to any other data point we have. We have a state that has detailed evidence, Florida. We see that although there is a huge rise in cases, they are almost all overwhelmingly healthy young people. They are not being hospitalized. They are not dying. The deaths are going down per day. The hospitalizations are going down per day. It’s just not likely.”
“I think that what is happening in Texas, I know that this is true, they are testing every person that gets hospitalized for Covid-19,” Atlas continued. “We know that the vast majority of people with COVID-19 who are young, particularly, are asymptomatic or minimally symptomatic. I question if those people who are positive for COVID-19 and being hospitalized for something else are classified as COVID-19 hospitalizations. That’s a big difference.”
Atlas went on to explain that younger people getting the infection is actually a good thing because it leads to herd immunity over the long term…….
[Dr. Robert Levin, Health Officer and Medical Director, Ventura County] He predicted 400-to-600 hospitalizations a day. He revised that to 200-to-400 a day…. we are barely over 200 for the ENTIRE ordeal…. We now have a panic over 51 total hospitalizations in a county with eight hospitals. Can you people do math? Can you PLEASE do basic math. This is not a crisis, you however, have created one. You, in an effort to try and prevent all deaths (we’ve had 43 deaths) you have ended all relevant life…. (See more at JOHN ZIEGLER’S site)
(A quick note, I am not saying we should have done nothing, please do not infer that from what is below. However, I am saying that pushing the shutting down of our infrastructure for anything past two or three weeks ~ is ~ dubious at best.)
As An Aside, this is one of the most important article I believe regarding this whole “pandemic” issue we are dealing with. While it focuses on New York City, this is multiplied ad infinitum around our nation and globe. I would highly recommend this article at CITY JOURNAL:
My computer is down, and its a brand new build (something I did surely found out it is a bad motherboard). But my phone is allowing me opportunity to expand on some thinking. In a conversation about reopening Minnesota I had the other morning. I will include the conversations end below the raw numbers and pics. Take note I start with my old numbers of THE RONA’S estimated infection rates, with newer studies, as well as some HERD IMMUNITY stats/commentary. Enjoy number crunchers. I will add some other Faceboook posts as well.
INFECTION RATES
This portion was the earliest idea to how widespread the virus was. People would continuously mention the KNOWN infection rate of Covid-19 to the KNOWN death rate from Covid. And then in the same breath compare those stats to the ESTIMATED flu infection rate to the SOMEWHAT KNOWN flu death rate. And then they would say “see, Covid-19 is more deadly.” But I wanted to compare the same stats… so this was my way of referenced “estimations” to the infection rate of Covid-19. These were the two referenced numbers:
There are probably 25 to 50 people who have the virus for every one person who is confirmed. (Dr. Makary BIO|YAHOO)
Now, as the testing for antibodies is getting under way, we are finding confirmation for the above numbers. Here are some articles to make the point (as well as some media) HERE ARE SOME IMPORTANT THINGS TO KEEP IN MIND regarding the Santa Clara County information….
Closer to the publishing date of the information garnered from the 3,300 volunteers getting the antibody test in Santa Clara County, there were 32-deaths attributed to the Coronavirus, or, THE RONA. So what we can assume is that as the death toll rises over a time-line, so does the infection rate. Here is what the REASON.COM ARTICLE notes closer to the studies publishing date:
Between 48,000 and 81,000 residents of Santa Clara County, California are likely to have already been infected by the coronavirus that causes COVID-19, suggests a new study by researchers associated with Stanford University Medical School. The researchers tested a sample of 3,330 residents of the county using blood tests to detect antibodies to determine whether or not they had been exposed to the coronavirus. If the researchers’ calculations are correct, that’s really good news. Why? Because that data will help public health officials to get a better handle on just how lethal the coronavirus is, and if researchers are right it’s a lot less lethal than many have feared it to be.
Currently, the U.S. case fatality rate, that is, the percent of people with confirmed diagnoses of COVID-19 who die, is running at 5.2 percent. But epidemiologists have known that a significant proportion of people who are infected are going undetected by the medical system because either they don’t feel sick enough to seek help or are asymptomatic. For example, recent research in Iceland suggests that about 50 percent of people infected with the virus have no symptoms.
In the new study, the researchers sought residents through Facebook to whom they could administer the antibody tests. The results were an unadjusted prevalence of coronavirus antibodies of 1.5 percent. After making various statistical and demographic adjustments, researchers calculated the likely prevalence ranged from 2.49 to 4.16 percent. At the time that these tests were administered, there were about 1,000 confirmed COVID-19 cases and 32* deaths from the disease in Santa Clara County. The upshot is that “these prevalence estimates represent a range between 48,000 and 81,000 people infected in Santa Clara County by early April, 50- 85-fold more than the number of confirmed cases.”
Using these data, the researchers calculated the infection fatality rate, that is, the percent of people infected with the disease who die: “A hundred deaths out of 48,000-81,000 infections corresponds to an infection fatality rate of 0.12-0.2%,” they report.* That’s about the same infection fatality rate the Centers for Disease Control and Prevention (CDC) estimates for seasonal influenza…..
COVID-19 Lethality Not Much Different Than Flu, Says New Study: Possible really good news from a population screening antibody test study in Santa Clara County, California (REASON | ABC NEWS)
Why A Study Showing That Covid-19 Is Everywhere Is Good News: If millions of people were infected weeks ago without dying, the virus must be less deadly than official data suggest (ECONOMIST)
Medical Experts Appear on ‘Life, Liberty, and Levin’ to Urge Leaders to Reopen America (PJ-MEDIA)
LA Study: Virus May Be More Widespread, Less Deadly Than Thought (NEWSMAX)
TWITTER: Andrew Bostom
@AlexBerenson “We find strong evidence that COVID-19 is widespread (>28 million) in the US but don’t panic.”
Yes. Reduces case-fatality ratio to ~0.1% https://t.co/DgmM1wDdqx
I mention to people that with all the precautions many states are forcing on its population they are retarding the rate of HERD IMMUNITY… which is important.
HERD IMMUNITY
Important because Dr. Fauci mentioned during one of his briefings that this is coming back in the winter season. But because we have chosen as a nation to not allow for normal contact that nature demands of us, we will be dealing with this at a higher rate than say Sweden.
Our governor, Gavin Newsom, thinks he “sounds” scientific — but has no idea [apparently] what or how to achieve “herd immunity.” Here is a MERCURY NEWS article discussing the issue statements by our “fearless” governor:
“The prospect of mass gatherings is negligible at best until we get to herd immunity and we get to a vaccine,” Newsom said. “So large-scale events that bring in hundreds, thousands, tens of thousands of strangers altogether across every conceivable difference, health and otherwise, is not in the cards based upon our current guidelines and current expectations.”
The article mentions no large gatherings until Thanksgiving… but then the flu and Covid-19 season starts again. Are we shutting down our economy (bars, restaurants, small businesses, etc) and flights, beaches, etc., in the 2020-2021 season? (THANKFULLY “Attorney General William Barr warned that states could find themselves in hot water from the Justice Department if their coronavirus lockdowns go ‘too far’.” | BREITBART)
Why Simply Waiting For Herd Immunity To Covid-19 Isn’t An Option: Waiting for enough people to catch the coronavirus could take a very long time (MIT TECH REVIEW)
Sweden Resisted A Lockdown, And Its Capital Stockholm Is Expected To Reach ‘Herd Immunity’ In Weeks (CNBC)
Sweden has allowed nature to provide a natural defense to future Covid-19 outbreaks. By doing so, the next time this comes around (2020-2021) Sweden will be the most prepared out of the Western Nations. Bravo Sweden, and they took the idea that destroying their economy was not the wisest of choices.
JOHN STOSSEL
UNCOMMON KNOWLEDGE BONUS
March 27th
April 17th
Steve and I agree on a lot, I do not wish to put Steve here in a bad light… he is a guy that I would probably enjoy conversation with over a beer or two (or three):
EXCERPT FROM FACEBOOK CONVO
(ME)
Steve W — you do know Steve that the same amount of death from and infection due to Covid-19 exists under the trend line of doing nothing and the most strict quarentine rules…. right? In other words, we are not saving lives. And, in fact, we have made it worse for our economy next fall/winter because it is coming back as it makes its rounds around the world.
(STEVE W)
Sean Giordano I have heard that said but not seen it from a credible source. So I think that is false.
(ME)
Steve W what is false?
(STEVE W)
Sean Giordano “the same amount of death from and infection due to Covid-19 exists under the trend line of doing nothing”
(ME)
Steve Wallace now you are saying don’t listen to Dr. Fauci?
Many bemoan Trump for not listening to him (even though he has), and some I meet do not support Fauci in the idea that this was to elongate the process as to not put any undue stress on our health care system. Even though he clearly announced multiple times this was the reason to do so
WORLD ECONOMIC FORUMmentions the following, and all the graphs of the United States shown by Doctors Fauci and Birx have all used this idea as well (graph below from CDC and WEF)
CHRIS WALLACE: All right. You talk about slowing the virus down. You talk a lot, and I’ve very used to this now, you can either have a bump like this of cases or you could make it maybe the same total cases, but it’s a much more gradual and slower and longer curve. I want to put up some numbers. We have in this country about 950,000 hospital beds, and about 45,000 beds in Intensive Care Unit. How worried are you that this virus is going to overwhelm hospitals, not just beds, but ventilators? We only have 160,000 ventilators. And could we be in a situation where you have to ration who gets the bed, who gets the ventilator?
DR. FAUCI: OK. So let me put it in a way that it doesn’t get taken out of context. When people talk about modeling where outbreaks are going, the modeling is only as good as the assumptions you put into the model. And what they do, they have a worst-case scenario, a best-case scenario, and likely where it’s going to be. If we have a worst-case scenario, we’ve got to admit it, we could be overwhelmed. Are we going to have a worst-case scenario? I don’t think so. I hope not.
What are we doing to not have that worst-case scenario? That’s when you get into the things that we’re doing. We’re preventing infections from going in with some rather stringent travel restrictions. And we’re doing containment and mitigation from within. So, at a worst-case scenario, anywhere in the world, no matter what country you are, you won’t be prepared. So our job is to not let that worst-case scenario happen.
(…. STILL ME….)
STEVE W for you not to understand the goal of all this, and then get on here sharing insights is itself insightful. I am not blaming you STEVE… I just see this fundamental misunderstanding of the underlying factors and goals of this whole endeavor of bending the curve as applicable to MANY A PERSON in these discussions here and elsewhere on social media. I am giving you, in fact, the most respectful benefit of a doubt, but am merely in conversation with you at this moment. This conversation is just multiplied (others are having) across social media many fold. Blessings to you and yours friend. Yet, this foundational view is not known well by others… that is, the reason behind flattening the curve as well as the data underneath the trend line.
(CLICK TO ENLARGE)
Here I wish to switch gears a bit and start to discuss another “info graphic” post from MY SITES FACEBOOK I shared with my readers. And since the entire idea behind “flattening the curve” was to keep the health and hospital system working well by not getting inundated all at once, this should have lasted two or three weeks. Not as long as it has — our economy is important too! Damnit!
CAPACITY OF THE HEALTHCARE SYSTEM
The following was compiled after a conversation I had on Facebook. It touches on some of the issues above. Enjoy
I note the bell curve because many are under the false impression we are doing this to “save lives.” This was never the case.
The quarantine was to lessen the apex of the bell curve as to not put pressure on the hospital/health system. The same amount of people in the elongated “quarantine bell curve” (the trend-line) would die and get sick. In other words, the same statistics exist below the line (POWERLINE). Here is a site cataloging the hospitalizations for the rona that POWERLINE used – US CORONAVIRUS HOSPITALIZATIONS …they used both the CDC site and this one, but the CDC site has lower hospitalizations, so they opted for the most updated numbers. WHICH AS OF APRIL 21ST STAND AT 84,292 HOSPITALIZATIONS FROM JANUARY TILL NOW. This is important, because, the flu season of 2017-2018 we saw 810,000 hospitalization, and our health system didn’t collapse. Nor did the Swine Flu of 2009-to-2010, which saw 60-million American infected and 300,000 hospitalizations.
This then may explain why all the field hospital’s the ARMY CORE OF ENGINEERS built are being dismantled without a single bed being used.
The panic and fear among the people who cannot be bothered to read the actual statistics about this pandemic is what should concern most preppers. In fact, this virus has been so overhyped that the Army’s field hospital in Seattle, an “epicenter” of the pandemic has closed after three days without seeing one single COVID-19 patient. According to a report by Military.com, the hastily built field hospital set up by the Army in Seattle’s pro football stadium is shutting down without ever seeing a patient. [….] The decision to close the Seattle field hospital comes amid early signs that the number of new cases could be hitting a plateau in New York, the epicenter of the coronavirus epidemic in the U.S., and other states. At a news conference Friday, New York Governor Andrew Cuomo said, “Overall, New York is flattening the curve.” — ZERO HEDGE (see: MILITARY TIMES | DAILY CALLER)
Unlike the Mercy, the Comfort is treating COVID-19 patients on board as well as patients who do not have the virus. The ship has treated more than 120 people since it arrived March 30, and about 50 of those have been discharged, said Lt. Mary Catherine Walsh. The ship removed half of its 1,000 beds so it could isolate and treat coronavirus patients. [The Mercy has seen 48 patients, all non-Covid related] (THE STAR)
And literally handfulls of patients on the Comfort (New York City) and the Comfort (Los Angeles) — *see comment below. There was never a shortage of respirators (NATIONAL REVIEW), and we may surpass the 2018-to-2019 flu death rate, but come nowhere close to the 2017-to-2018 flu death rate:
(CLICK TO ENLARGE)
And it seems that we are reaching a plateau with The Rona, so there is good news in this regard (POWERLINE).
* Here is a comment from the Military Times article from a few days ago:
So, why did we spend all that Taxpayer’s money to move the Comfort to NYC and all the added Military medical personnel to staff the Javitt’s Center? Because Cuomo was crying WOLF.
“So far, the thousands of beds provided by a converted convention center and a hospital ship have not been needed, but the extra personnel are coming in handy for the city’s civilian hospitals.
About 200 doctors, nurses, respiratory therapists and others are working in New York’s medical centers, where bed space has not been overwhelmed, but where hospital-acquired coronavirus cases have sidelined civilian staff.”
Dr. Drew’s beyond fed up with the media coverage of the coronavirus, because he believes it’s majorly overblown and causing hysteria … while another major threat’s being ignored.
Dr. Drew talks with CBS Local’s DJ Sixsmith about coronavirus, the media’s response to it, and why we shouldn’t be freaking out about it.
First a post by ACE OF SPADES, with a large excerpt from the NY POST article:
The breathless reporting from pretty much every source, with the exception of Michael Fumento in the NY Post is typical of the no-nothings in the media and their tenuous relationship with logic and the Scientific Method and pesky little things like data and numbers and statistics.
And the facts are very, very thin. We don’t know much other than what the Chinese government is telling the world, and I believe them about as much as I believe that Epstein killed himself. Maybe it’s worse than they are reporting. Maybe it is overblown to deflect attention from other things in China, like Hong Kong! And maybe it is just like most of the other diseases that emerge from China and then fizzle in developed countries because we are healthier, cleaner, have better medical care and more efficient ways to get that care to the people who need it.
I have no idea how this will shake out. Is it the next pandemic, with hundreds of millions dead? Maybe, but I doubt it. Is it the next SARS? Probably. And how many Americans died of SARS? From the CDC:
In the United States, only eight persons were laboratory-confirmed as SARS cases. There were no SARS-related deaths in the United States. All of the eight persons with laboratory-confirmed SARS had traveled to areas where SARS-CoV transmission was occurring.
For all of American medicine’s faults, we do a pretty good job of minimizing the severity of things like the flu and TB and Measles and Pertusis and all sorts of diseases that are major killers in other parts of the world. Will I take a trip to Wuhan? hell no. But until there is evidence of this virus being a significant health threat in the developed world I will not worry too much.
A CNN reporter broadcasts from Wuhan, China, on the recent viral outbreak. There is nobody near who could possibly infect him — unless the cameraman has Guinness Book of Records coughs and sneezes. So why does he insist on wearing a blue surgical mask while talking?
It’s called “drama,” which is badly needed, because there appears to be nothing very special about this outbreak of the 2019-nCoV or Wuhan virus. It should actually be called the DvV, or Déjà vu Virus, because we have been through these hysterias before. Over and over. Heterosexual AIDS, Ebola repeatedly, the H1N1 swine flu that was actually vastly milder than the regular flu and, especially, severe acute respiratory syndrome (SARS) in 2003.
Once you start debunking mass hysteria over outbreaks, it gets easy, because the same patterns repeat themselves.
The best remedy for all epidemic hysteria is perspective. How is this new outbreak different and thus potentially more dangerous from other diseases we have dealt with in the past or are dealing with now?
Wuhan is repeatedly labeled “deadly” — but so is every other virus most people know about. But especially deadly? Nearly 600 cases have been confirmed with at least 17 reported deaths.
[….]
What we can say for sure is that Wuhan will be a lot worse in China, simply because health care there is vastly inferior. It appears that, like flu, Wuhan usually kills through often treatable secondary infections. Well, treatable in the West. You’d be surprised at how many potentially deadly diseases (malaria, TB) Americans get that wreak havoc in much of the world but kill essentially none of us.
It also appears those most likely to die of Wuhan virus fit the same profile as flu fatalities: people over 65, those with compromised immune systems and those with serious pre-existing conditions. Two of the 17 Wuhan dead were 89-year-olds with pre-existing conditions; the youngest was 48 and suffering from diabetes and a stroke.
Contagiousness is highly important, of course. But so far, there is no evidence that Wuhan, first reported more than three weeks ago, is more contagious than influenza or spreads differently.
Those are the important factors; everything else is noise and tinfoil-hat paranoia.
[….]
It’s inherently bad because it’s new, we’re told. So were swine flu and SARS.
Chinese health officials warned it could mutate further to either become more deadly or more contagious. Same was said about the aforementioned outbreaks. Actually, viruses usually mutate to become less deadly, to preserve the host body and hence themselves.
The media are correct in saying the closest comparison here is SARS. It also was first reported in China and was what’s called a coronavirus. But while they want you to remember SARS as akin to the Black Death with cries of “Bring out your dead!,” fact is, there was a grand total of only 8,098 cases, of whom 774 died. Then the disease simply disappeared. More than 7,000 of those cases and about 650 of the deaths occurred just in mainland China and Hong Kong. The United States had just 75 cases and zero deaths.
By contrast, the CDC estimates about 80,000 Americans died of flu two seasons ago.
So if you want, buy a (probably worthless) surgical mask to play “twins” with those “courageous” TV newsmen. Or you may consider that flu shots are still available.
(Originally posted in 2014) I know facts can be the killjoy to personal feelings and beliefs… trust me, I know. However, here and now I wish to tread on the “good feelings” one gets from the belief in silly things heard of but never checked out. Often this deals with things like political positions and religious beliefs… but here I wade into the pet-owner world.
Firstly I wish to deal with a myth I just recently heard that dogs saliva heal your wounds well. This is a myth! Here for instance is some great veterinary info on the topic… and after reading it I may actually shoo dogs away from doing this:
DOG SALIVA GOOD FOR HUMANS
It’s not likely that your dog will pass on any illnesses to you through its saliva. Many of the bacteria in your dog’s saliva is specific to canines, and won’t harm you. However, it’s a good idea to discourage licking to reduce any chances of becoming sick from germs. Here are some myths about dog saliva and their associated facts.
Myths About Dog Saliva
Because dog saliva contains a special enzyme which promotes healing of the dog’s wound, some pet owners think it will have the same effect on their own cuts. The enzymes in your dogs saliva only work on the wounds of dogs. Allowing your dog to lick your cuts could lead to infection from any germs the dog may have in its mouth.
Facts About Dog Saliva
One potential health risk associated with being licked by your dog is the transmission of roundworms. These intestinal parasites are commonly found in kittens and puppies and are passed through licking. Symptoms of roundworm are coughing, a fever and headaches. Of course if your dog has been given deworming medication, and is tested on a regular basis, your risk of contracting roundworm is slim. Leptospirosis, salmonella and E. coli are other illnesses that can be transmitted by your dog’s saliva; ….
One site even goes as far as to warn that “People with weakened immune systems and young children probably should not have direct contact with dog or cat saliva.” So, strike that ol’ wives tale, bottom line is this:
Some people believe that the dogs’ saliva can heal the wounds as well. It is absolutely wrong. Dogs are different specie with diverse specifications. Their saliva is useful for them and but not for humans….
One dog saliva myth is that it’s beneficial both for dog wounds and human wounds. There is a bit of truth in this belief, but putting dog saliva on a human wound can result in any number of problems. The bacteria in the saliva may infect a human’s skin and prove to be harmful for the human. (DogsHealth.com)
Here is an updated story for your purview via PJ-MEDIA:
A Wisconsin man has lost both of his legs due to an infection that he caught from a dog. Greg Manteufel was reportedly licked by his own pet. As a result, a bacterial infection called capnocytophaga raged through his body and wreaked havoc.
Initially, Manteufel thought that he had the flu. He went to the emergency room, and was so covered in bruises that it looked as if he had been beaten. Blood tests soon revealed the cause of his symptoms. His body’s response to the bacteria “caused Greg’s blood pressure to drop, and the circulation in his limbs to decrease rapidly,” according to ABC7.
“Sometimes it decreases so much that the arms and legs just die,” Dr. Munoz-Price of Froedtert Hospital and the Medical College of Wisconsin said…
.
HYPOALLERGENIC DOGS
Okay, let us move onto “hypoallergenic dogs.” This is another myth born from my wife going into sneezing/stuffy nose fits at a co-workers house with poodles. She mentioned that her dogs are “hypoaalergenic.” I too thought this was a breed that would in the least cut down on my wife’s reaction to the dog. Upon further study, I was wrong. Here is the Globe and Mail comments on a recent study:
Forget about that labradoodle: A new report suggests household allergens are no lower in homes that keep hypoallergenic dogs versus hairier, dander-heavy breeds.
“We found no scientific basis to the claim hypoallergenic dogs have less allergen,” senior author Christine Cole Johnson said in a release.
“Exposure to a dog early in life provides protection against dog allergy development. But the idea that you can buy a certain breed of dog and think it will cause less allergy problems for a person already dog-allergic is not borne out by our study,” said Dr. Johnson, who chairs the Department of Public Health Sciences at Detroit’s Henry Ford Hospital.
And this from HuffPo, via Dr. Karen Becker (Proactive and integrative wellness veterinarian):
A 2011 study published in The American Journal of Rhinology and Allergy reveals the amount of dog allergens found in households with dogs does not vary depending on the breed. In other words, families with so called “hypoallergenic” dogs are living with the same level of allergens in their homes as people who own non-hypoallergenic canines.
Study researchers measured the level of the most common dog allergen, Canis familiaris 1, or Can f 1, found in the homes of 173 families that owned one dog. Out of the 173 samples, only 10 had less than measurable amounts of Can f 1. No matter what type of dog was in the home, there was no significant difference in the level of allergens measured.
No One Knows How the Myth of Allergy-Free Dogs Got Started
“I have no idea where this whole concept came from. It’s been around a long time, and maybe people associated it with shedding. I think it’s just a legend,” says Dr. Christine Cole Johnson, an epidemiologist at Henry Ford Hospital in Detroit and senior author of the study.
The scientists who conducted the study discovered 60 of 161 recognized breeds were named as hypoallergenic on various Internet websites. However, there is no official list of hypoallergenic breeds, though the American Kennel Club (AKC) does suggest 11 canine candidates for people with allergies. The kennel club only suggests certain breeds might be beneficial for allergy sufferers — it doesn’t recommend or endorse any specific breed.
No matter how they did their comparisons, the scientists found no statistically significant differences in the levels of Can f 1 in dust samples in those 163 homes. (National Institutes of Health)
So these two oft repeated statements of fact by many are merely wives tales passed on by those that love animals so much that their critical thinking skills are suspended. And while I think the video below is cute as hell… is someone asked me the following: “My dog licks my babies in the face, should I make him/her stop?”
BEST ANSWER:
There are several thousand cases of children going blind from hookworm infections that are passed to their eyes from dogs every year. [Cats too!] Children can also be infected with hookworms from dogs licking them in the face if the dog is infected. The most common bacterial infection that causes GI upset in humans resides in dogs’ mouths.
We actually have a brochure at work that we give to parents about infection that can be passed from dogs to children via dogs’ mouths, and before we started giving out the brochure, we actually had a client whose daughter got hookworms from their dog.
If it were me, I’d make the dog stop liking the child’s face and train it to lick other places (or to just not lick at all…)
Morgan Spurlock admitted something that cast more doubt onto his lauded documentary entitled “Super Size Me” to which an excellent documentary response already noted the secrecy behind Spurlocks health records, “Fat Head.” Here are a couple article’s noting Phelim McAleer’s article in the Wall Street Journal entitled, “A Big Mac Attack, or a False Alarm?,” which Dennis Prager reads from:
Morgan Spurlock’s Alcoholism Confession Casts Doubt on His ‘Super Size Me’ Health Claims (BREITBART)
Super-Size My Doubts About Morgan Spurlock’s Snide Documentary About McDonald’s (AMERICAN THINKER)
Rush Limbaugh dismantles a lie from the Left expressed by Jimmy Kimmel’s monologue regarding Trump’s first few days in office and his rescinding an Obama era bill that was an Executive Order.
If the Left do not like this legal snafu of one President rescinding another’s E.O., pass laws through Congress dammit! U-n-l-e-s-s they just want to u-s-e the controversy to support their wild positions that have no reality in the real world. Here are the organizations who supported Trump’s action (via the WASHINGTON FREE BEACON):
…Officials at the American Civil Liberties Union opposed the rule and called for its repeal because the process did not include sufficient due process protections.
“The rule includes no meaningful due process protections prior to the SSA’s transmittal of names to the NICS database,” the group said in their letter. “The determination by SSA line staff that a beneficiary needs a representative payee to manage their money benefit is simply not an ‘adjudication’ in any ordinary meaning of the word. Nor is it a determination that the person ‘[l]acks the mental capacity to contract or manage his own affairs’ as required by the NICS. Indeed, the law and the SSA clearly state that representative payees are appointed for many individuals who are legally competent.”
On behalf of the American Civil Liberties Union (ACLU), we urge members of the House of Representatives to support the resolution disapproving the final rule of the Social Security Administration which implements the National Instant Criminal Background Check System Improvement Amendment Acts of 2007….
…In December 2016, the SSA promulgated a final rule that would require the names of all Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) benefit recipients – who, because of a mental impairment, use a representative payee to help manage their benefits – be submitted to the National Instant Criminal Background Check System (NICS), which is used during gun purchases.
We oppose this rule because it advances and reinforces the harmful stereotype that people with mental disabilities, a vast and diverse group of citizens, are violent. There is no data to support a connection between the need for a representative payee to manage one’s Social Security disability benefits and a propensity toward gun violence. The rule further demonstrates the damaging phenomenon of “spread,” or the perception that a disabled individual with one area of impairment automatically has additional, negative and unrelated attributes. Here, the rule automatically conflates one disability-related characteristic, that is, difficulty managing money, with the inability to safely possess a firearm.
The rule includes no meaningful due process protections prior to the SSA’s transmittal of names to the NICS database. The determination by SSA line staff that a beneficiary needs a representative payee to manage their money benefit is simply not an “adjudication” in any ordinary meaning of the word. Nor is it a determination that the person “[l]acks the mental capacity to contract or manage his own affairs” as required by the NICS. Indeed, the law and the SSA clearly state that representative payees are appointed for many individuals who are legally competent…
…[R]egulation of firearms and individual gun ownership or use must be consistent with civil liberties principles, such as due process, equal protection, freedom from unlawful searches, and privacy. All individuals have the right to be judged on the basis of their individual capabilities, not the characteristics and capabilities that are sometimes attributed (often mistakenly) to any group or class to which they belong. A disability should not constitute grounds for the automatic per se denial of any right or privilege, including gun ownership.
So, if you donated the ACLU after President Trump’s executive travel ban, congratulations. Yesterday’s vote was your victory, too…..
The WASHINGTON TIMES also brings some historical clarity to the issue:
In recent years, advocates for the mentally ill created more boundaries for law enforcement and healthcare workers to forcibly hospitalize Americans who are suspected of being a danger to both themselves and others. The 1966 Lanterman Petris Short Act (LPS Act) was California legislation designed to reform the antiquated state of mental institutions in the state.
It should be noted that LPS was signed by Governor Reagan in California but only after pressure from groups like the ACLU stepped in and sued on behalf of patients who were being involuntarily hospitalized. Other states followed suit with their own similar involuntary and voluntary commitment statutes.
According to U.S. Veteran’s Affairs, “Maurice Rodgers, spokesman for the California State Psychological Association, called the plan the “Magna Carta of the Mentally Ill,” while the American Civil Liberties Union (ACLU), officially in support of the legislation, raised objection to the fact that the patient had to personally petition for a due process hearing at the initial point in the commitment.
….Later, the Carter administration signed into law the Mental Health Systems Act of 1980, which largely promoted the same idea for national facilities. In 1981, when both parties in Congress agreed to the Omnibus Budget Reconciliation Act of 1981, President Reagan signed that into law. One of it many provisions was to eliminate federal funding for community services and thereby transfer funding back to individual funding or state-funded efforts. Had Reagan even been aware of that part of the Act, he would have immediately realized the Act was negating the disastrous effects of the LPS he experienced as governor of California.
In other words, the State needs more funding control over mental health facilities, whether local, community, or state. Serious cases could still be funded through Medicaid, creating a virtual federal funding pool of money. This was formalized in the Mental Health Planning Act of 1986.
In effect, bipartisan policies recommended that the Federal government transfer government funding of community mental health facilities back to the states. State-funded facilities as well as privately-funded facilities were not affected by that policy. Reagan signed the bill into law as part of an overall spending cut package. As he would have known, complete state funding of facilities resulted in terrible mental healthcare, but state governments had an obligation to provide for this. However, in 1986, he also signed into a law another bipartisan solution to have Medicaid assist with funding. The laws closed not a single facility.
Ergo, to the liberals, REAGAN CLOSED THE MENTAL HEALTH FACILITIES. The fact that states closed some facilities and let staff go at others due to their own budget issues is unimportant because, of course, liberals hated Reagan. And still do.
[…..]
So when you hear the argument that Reagan closed the mental health facilities, ask the name of one health facility that Reagan actually closed. And when it closed. And how he closed it. And if you hear that Reagan closed it by extenuation of a funding cut, ask which particular bill he signed into law specified that particular facility be closed.
Or is it a case that bipartisan governments at the state and federal levels attempted to improve healthcare treatment and that bipartisan governments within the states screwed things up so badly that individual departments of health closed down less effective facilities? You will have lost the typical liberal at the word bipartisan….
A lifelong Democrat at the DAILY JOURNAL LETTERS ties this all in a neat bow for us:
…As a lifelong Democrat (of the Irish-Catholic-Labor variety), I think Reagan did some good things and other things I didn’t support. But one thing Reagan didn’t do was single-handedly “close down” mental hospitals thus triggering 40 years of mental health hell.
Two other forces actually determined the fate of mental health care in this state. You might call them acts with unintended consequences. Here’s the history.
In 1967, the Lanterman-Petris-Short Act (LPS Act) a so-called “bill of rights” for those with mental health problems passed the Democratic-controlled Assembly: 77-1. The Senate approved it by similar margins. Then-Gov. Reagan signed it into law.
It was co-authored by California State Assemblyman Frank Lanterman, a Republican, and California State Senators Nicholas C. Petris and Alan Short, both Democrats. LPS went into full effect on July 1, 1972.
The bipartisan law came about because of concerns about the involuntary civil commitment to mental health institutions in California. At the time, the act was thought by many to be a progressive blueprint for modern mental health commitment procedures, not only in California, but in the United States.
Its main purposes were:
To end the inappropriate, indefinite, and involuntary commitment of mentally disordered persons, people with developmental disabilities, and persons impaired by chronic alcoholism, and to eliminate legal disabilities;
To provide prompt evaluation and treatment of persons with serious mental disorders or impaired by chronic alcoholism;
To guarantee and protect public safety;
To safeguard individual rights through judicial review;
To provide individualized treatment, supervision, and placement services by a conservatorship program for gravely disabled persons;
To encourage the full use of all existing agencies, professional personnel and public funds to accomplish these objectives and to prevent duplication of services and unnecessary expenditures;
To protect mentally disordered persons and developmentally disabled persons from criminal acts.
Initially, mental health advocates pushed for community-based mental health facilities that would replace the closed mental hospitals.
But that never happened because even though post-Reagan the legislature was still controlled by Democrats, no major funding for new community-based mental health facilities ever occurred. And that situation basically is still the case today.
The second force at work in the mental health care issue were the courts and what is known as “deinstitutionalization.”
During the 1960s, many people began accusing state mental hospitals of violating the civil rights of patients. Some families did, of course, commit incorrigible teenagers or eccentric relatives to years of involuntary confinement and unspeakable treatment. Nurse Ratched, the sadistic nurse famously portrayed in the book and film “One Flew Over The Cuckoo’s Nest,” became a symbol of institutional indifference to the mentally ill.
By the late 1960s, the idea that the mentally ill were not so different from the rest of us, or perhaps were even a little bit more sane, became trendy. Reformers dreamed of taking the mentally ill out of the large institutions and housing them in smaller, community-based residences where they could live more productive and fulfilling lives.
A mental patient could be held for 72 hours only if he or she engaged in an act of serious violence or demonstrated a likelihood of suicide or an inability to provide their own food, shelter or clothing due to mental illness. But 72 hours was rarely enough time to stabilize someone be held another two weeks for evaluation and treatment.
As a practical matter, involuntary commitment was no longer a plausible option…..