
Jump To
June 27th
- Stanford Study — to the left and below
- (matches closely my March numbers)
- Can You Contract Twice?
- Can Animals Contract and Spread?
June 19th
May 24th
STANFORD has released a new paper where they look at their own studies as well as “23 studies with a sample size of at least 500 have been published either in the peerreviewed literature or as preprints as of June 7, 2020.” In this they find confirmation to strongly say:
…In the paper, which has not yet been peer-reviewed, Ioannidis surveyed 23 different seroprevalence studies and found that “among people <70 years old, infection fatality rates ranged from… 0.00-0.23% with median of 0.04%.”
The median fatality rate of all cases, he writes, is 0.26%, significantly lower than some earlier estimates that suggested rates as high as over 3%.
In the paper, Ioannidis acknowledges that “while COVID-19 is a formidable threat,” the apparently low fatality rate compared to earlier estimates “is a welcome piece of evidence.”
“Decision-makers can use measures that will try to avert having the virus infect people and settings who are at high risk of severe outcomes,” he writes. “These measures may be possible to be far more precise and tailored to specific high- risk individuals and settings than blind lockdown of the entire society.”
MY NUMBERS
Keep in mind in March I noted that the rates would be from 0.03% to 0.25% — not to brag or anything, but I am in the 23-studies lane-lines. I just couldn’t differentiate between age groups, but that was assumed as the average age of deaths.
And as states are going over death certificates, they are dropping by at least 25% in deaths by Covid-19. And some independent groups are helping “catch” the inflated number, like Pennsylvania’s “Wolf administration was caught this week adding up to 269 fake deaths to the state totals on Tuesday” (CITADELPOLITICS). Or this short example (PJ-MEDIA)
- On Thursday, the Washington State Department of Health (DOH) confirmed a report by the Freedom Foundation that they have included those who tested positive for COVID-19 but died of other causes, including gunshot injuries, in their coronavirus death totals. This calls into serious question the state’s calculations of residents who have actually died of the CCP pandemic.
- Last week, after it was reported that, like Washington, Colorado was counting deaths of all COVID-19 positive persons regardless of cause (which had resulted in the inclusion of deaths from alcohol poisoning), the Colorado Department of Health and Environment began to differentiate between deaths “among people with COVID-19” and “deaths due to COVID-19.”
Just one more of the many examples I could share is the New York Times getting 40% wrong of their “died from Covid-19 under 30-years old” front page news story. Mmmm, no, they didn’t die of Covid. As states figure this out, the inflated counts (like when Colorado did this — fell by 25%: lots more on this below).
CONTRACTED TWICE?
In a recent conversation two items came up that are worth updating for friends and family. The first deals with if a person can get the WuFlu twice. FORBES has a good article on this:
…Whenever I lecture on the Covid-19 outbreak, someone always asks me, “Can I get infected twice?” This is a natural concern. After all, if someone suffers through the prolonged fever, hacking cough, and profound weakness and misery caused by the virus, one small positive aspect might be not having to suffer through it a second time.
Such fears were ratcheted up after there were reports in Korea about people who had recovered from illness and tested negative, only to have a later test come up positive again. This prompted fear of new spread, even from recovered victims. Back in early March, a mayor in Texas, blasted the CDC for releasing a recovered patient from isolation, only to have that patient test positive again after release.
As a health care provider, the last thing you want to do is tell someone they are cured and release them back into the community, only to learn later that they started a whole new chain of virus transmission. Fortunately, a new study from the South Korean Center for Disease Control helps to answer part of the question. They studied patients who tested negative upon recovery, but in later tests became positive again. Could they spread the virus again?
It turns out, despite the positive test, they found that none of them were secreting live, infectious virus. It was a quirk of the rapid tests, which sample for low levels of genetic material, not whole virus. They concluded that the recovered patients had residual genetic fragments that still triggered the tests to turn positive. Those individuals were no longer contagious.
This was a relief. In other good news, a new draft paper reports that monkeys that were infected with the SARS-CoV-2 virus developed antibodies and were protected from illness when exposed to the virus a second time. It’s a small study, but it offers a glimmer of hope that once infected, there is immunity to re-infection….
The second issue was regarding animals being able to contract the virus.
ANIMALS
CNN has a good short response to this:
Q: Could I infect my pets with coronavirus, or vice versa? Can someone get infected by touching an animal’s fur? Should I get my pet tested for coronavirus?
A: There have been some reports of animals infected by coronavirus — including two pets in New York and eight big cats at the Bronx Zoo.
Most of those infections came from contact with people who had coronavirus, like a zoo employee who was an asymptomatic carrier.
But according to the CDC, there is no evidence animals play a significant role in spreading the virus to humans. Therefore, at this time, routine testing of animals for Covid-19 is not recommended.
As always, it’s best to wash your hands after touching an animal’s fur and before touching your face. And if your pet appears to be sick, call your veterinarian.
More “known” examples from the CDC:
- A small number of pet cats and dogs have been reported to be infected with the virus in several countries, including the United States. Most of these pets became sick after contact with people with COVID-19.
- Several lions and tigersexternal icon at a New York zoo tested positive for SARS-CoV-2 after showing signs of respiratory illness. Public health officials believe these large cats became sick after being exposed to a zoo employee who was infected with SARS-CoV-2. All of these large cats have fully recovered.
- SARS-CoV-2 was recently discovered in mink (which are closely related to ferrets) on multiple farms in the Netherlands. The mink showed respiratory and gastrointestinal signs; the farms also experienced an increase in mink deaths. Because some workers on these farms had symptoms of COVID-19, it is likely that infected farm workers were the source of the mink infections. Some farm cats on several mink farms also developed antibodies to this virus, suggesting they had been exposed to the virus at some point. Officials in the Netherlands are investigating the connections between the health of people and animals as well as the environment on these mink farms.
(The below is from June 19th)
COMPARED
MAROON numbers are death rate, and the BLUE numbers are hospitalization rates. Rated by placement as well. This is merely for comparison to decide if $1.1 trillion lost for every month of the economic shutdown and the long-term damage on the U.S. economy, shrinking it by $7.9 trillion over the next decade.
- [1] The 1918-19 “Spanish Flu” Pandemic — 675,000 died in the United States, some victims died within mere hours or days of developing symptoms.
- [2] The 1957-58 “Asian Flu” Pandemic — 116,000 deaths were in the US. Most of the cases affected young children.
- [3] The 1968 “Hong Kong Flu” Pandemic — 100,000 deaths occurred in the United States
- [12](9) The 2009 H1N1 Pandemic — About 80% of those deaths are believed to have been people younger than 65 — which is unusual. During typical seasonal influenza epidemics, 70-90% of deaths occur in people over 65. 274,000 hospitalizations, and 12,469 deaths in the United States due to the virus.
- [9](7) 2010-2011 flu season — 290,000 influenza-related hospitalizations and 37,000 flu-associated deaths
- [6](3) 2012-2013 flu season — 56,000 deaths is the CDC estimate. 571,000 influenza-related hospitalizations
- [8](6) 2013-2014 flu season — 347,000 influenza-related hospitalizations, and 38,000 flu-associated deaths
- [7](2) 2014-2015 flu season — 591,000 influenza-related hospitalizations, and 51,000 flu-associated deaths
- [11](8) 2015-2016 flu season — 280,000 influenza-related hospitalizations, and 23,000 flu-associated deaths
- [8](4) 2016-2017 flu season — 500,000 influenza-related hospitalizations, and 38,000 influenza-associated deaths
- [5](1) 2017-2018 flu season — The CDC estimates that between 46,000 and 95,000 Americans died due to influenza during the 2017-18 flu season. This resulted in an estimated 959,000 hospitalizations and a middle-ground of 61,099 deaths.
- [10](5) 2018-2019 flu season — 490,600 hospitalizations, and 34,200 deaths from influenza
- [4](10) Covid-19 (SARS-CoV-2) — With the adjusted numbers that I believe the flu (a bad influenza season assumed to be novel influenza on untested patients), I would bet we are at about 80,000 or less deaths from The WuFlu. US Coronavirus Hospitalizations is at a current level of 229,212.
Steven Crowder takes to the streets of Dallas to have real conversations with real people. In this installment, Steven discusses the COVID19 death count and the fake news surrounding it.
Crowder is posted above as an UPDATE to support my contention below:
(The below is from May 24th, 2020)
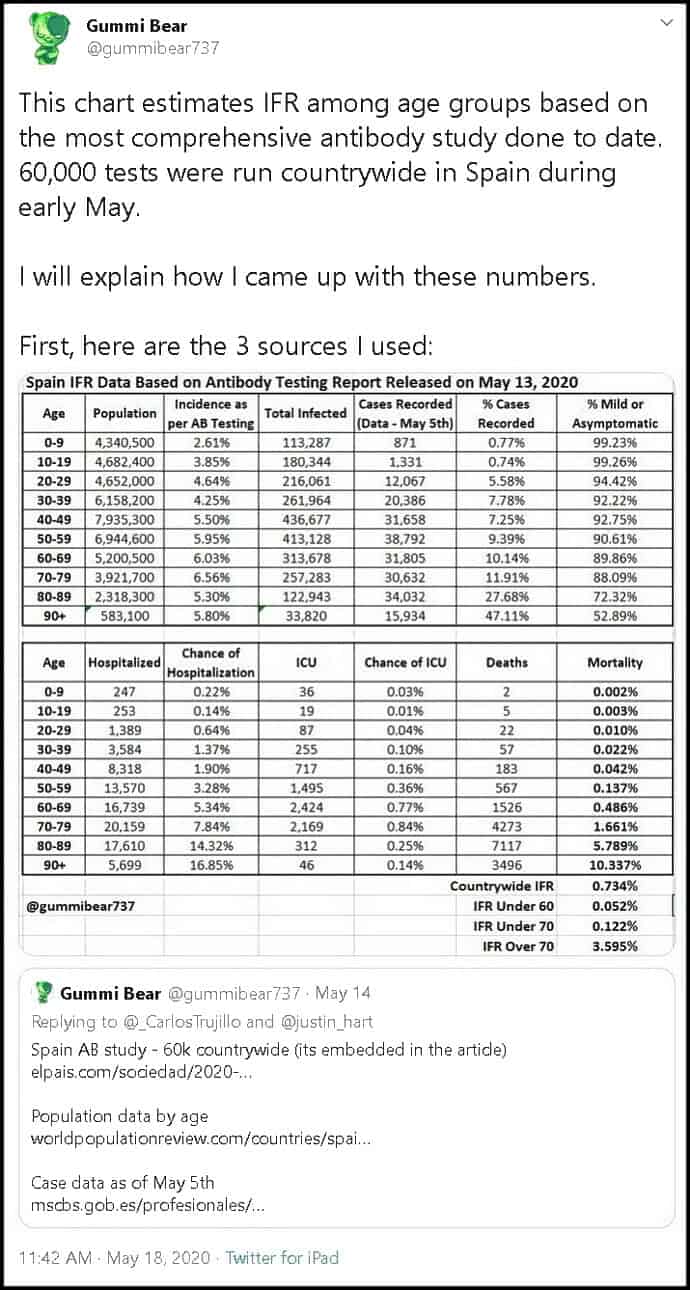
Here are some updated numbers, from CONSERVATIVE REVIEW — and I will post a portion of an older post [recently updated] underneath this (also, if the graphics are not linked to ENLARGE, I will link to the Twitter accounts associated with the graphics):
The CDC just came out with a report that should be earth-shattering to the narrative of the political class, yet it will go into the thick pile of vital data and information about the virus that is not getting out to the public. For the first time, the CDC has attempted to offer a real estimate of the overall death rate for COVID-19, and under its most likely scenario, the number is 0.26%. Officials estimate a 0.4% fatality rate among those who are symptomatic and project a 35% rate of asymptomatic cases among those infected*jump, which drops the overall infection fatality rate (IFR) to just 0.26% — almost exactly where Stanford researchers pegged it a month ago.


Until now, we have been ridiculed for thinking the death rate was that low, as opposed to the 3.4% estimate of the World Health Organization, which helped drive the panic and the lockdowns. Now the CDC is agreeing to the lower rate in plain ink.
Plus, ultimately we might find out that the IFR is even lower because numerous studies and hard counts of confined populations have shown a much higher percentage of asymptomatic cases. Simply adjusting for a 50% asymptomatic rate would drop their fatality rate to 0.2% – exactly the rate of fatality Dr. John Ionnidis of Stanford University projected.
More importantly, as I mentioned before, the overall death rate is meaningless because the numbers are so lopsided. Given that at least half of the deaths were in nursing homes, a back-of-the-envelope estimate would show that the infection fatality rate for non-nursing home residents would only be 0.1% or 1 in 1,000. And that includes people of all ages and all health statuses outside of nursing homes. Since nearly all of the deaths are those with comorbidities.
The CDC estimates the death rate from COVID-19 for those under 50 is 1 in 5,000 for those with symptoms, which would be 1 in 6,725 overall, but again, almost all those who die have specific comorbidities or underlying conditions. Those without them are more likely to die in a car accident. And schoolchildren, whose lives, mental health, and education we are destroying, are more likely to get struck by lightning.
[….]
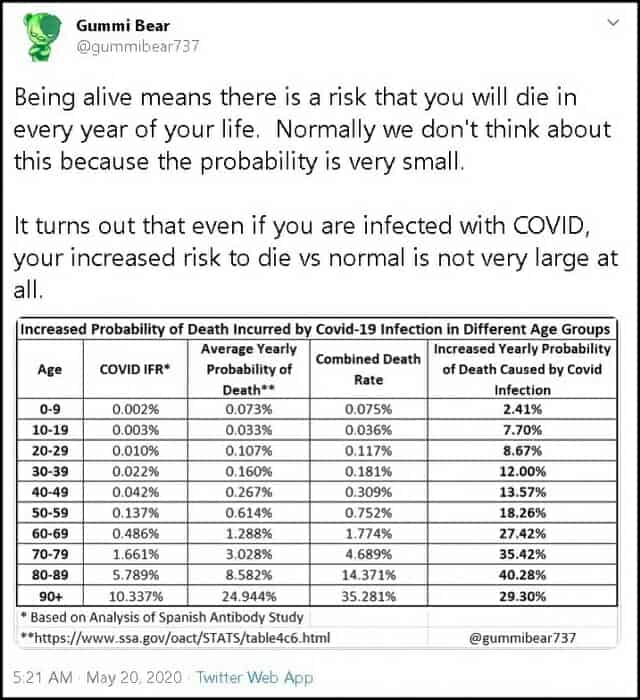
To put this in perspective, one Twitter commentator juxtaposed the age-separated infection fatality rates in Spain to the average yearly probability of dying of anything for the same age groups, based on data from the Social Security Administration. He used Spain because we don’t have a detailed infection fatality rate estimate for each age group from any survey in the U.S. However, we know that Spain fared worse than almost every other country. This data is actually working with a top-line IFR of 1%, roughly four times what the CDC estimates for the U.S., so if anything, the corresponding numbers for the U.S. will be lower.
FURTHER TWITTER DEBATE
I wanted to expand the Twitter graphic and link above a bit, I spent some time going through the comments and many of the conversational offshoots. I figured this collection (ending with my comment) sums up the issue in a lot less time:
(Click once to get large graphic, click again to blow it up)

There is a fascinating “official” continuation of this convo with more detail (linked in below Twitter graphic):
Great, great stuff. All this vindicates my own early numbers,
…all the “anti-body” studies,
…this more recent stuff,
…as well as all the Facebook discussions/debates between myself, friends, family, and complete strangers.
...AND,
…as I show below, this number will get lower upon investigation of common sense assumptions if never investigated.
REASON has their article discussing the issue of IFR and America compared to Europe (see also BLOOMBERG’S article):
According to the Centers for Disease Control and Prevention (CDC), the current “best estimate” for the fatality rate among Americans with COVID-19 symptoms is 0.4 percent. The CDC also estimates that 35 percent of people infected by the COVID-19 virus never develop symptoms. Those numbers imply that the virus kills less than 0.3 percent of people infected by it—far lower than the infection fatality rates (IFRs) assumed by the alarming projections that drove the initial government response to the epidemic, including broad business closure and stay-at-home orders.
The CDC offers the new estimates in its “COVID-19 Pandemic Planning Scenarios,” which are meant to guide hospital administrators in “assessing resource needs” and help policy makers “evaluate the potential effects of different community mitigation strategies.” It says “the planning scenarios are being used by mathematical modelers throughout the Federal government.”
The CDC’s five scenarios include one based on “a current best estimate about viral transmission and disease severity in the United States.” That scenario assumes a “basic reproduction number” of 2.5, meaning the average carrier can be expected to infect that number of people in a population with no immunity. It assumes an overall symptomatic case fatality rate (CFR) of 0.4 percent, roughly four times the estimated CFR for the seasonal flu. The CDC estimates that the CFR for COVID-19 falls to 0.05 percent among people younger than 50 and rises to 1.3 percent among people 65 and older. For people in the middle (ages 50–64), the estimated CFR is 0.2 percent.
That “best estimate” scenario also assumes that 35 percent of infections are asymptomatic, meaning the total number of infections is more than 50 percent larger than the number of symptomatic cases. It therefore implies that the IFR is between 0.2 percent and 0.3 percent. By contrast, the projections that the CDC made in March, which predicted that as many as 1.7 million Americans could die from COVID-19 without intervention, assumed an IFR of 0.8 percent. Around the same time, researchers at Imperial College produced a worst-case scenario in which 2.2 million Americans died, based on an IFR of 0.9 percent.
Such projections had a profound impact on policy makers in the United States and around the world. At the end of March, President Donald Trump, who has alternated between minimizing and exaggerating the threat posed by COVID-19, warned that the United States could see “up to 2.2 million deaths and maybe even beyond that” without aggressive control measures, including lockdowns.
One glaring problem with those worst-case scenarios was the counterfactual assumption that people would carry on as usual in the face of the pandemic—that they would not take voluntary precautions such as avoiding crowds, minimizing social contact, working from home, wearing masks, and paying extra attention to hygiene. The Imperial College projection was based on “the (unlikely) absence of any control measures or spontaneous changes in individual behaviour.” Similarly, the projection of as many as 2.2 million deaths in the United States cited by the White House was based on “no intervention”—not just no lockdowns, but no response of any kind.
Another problem with those projections, assuming that the CDC’s current “best estimate” is in the right ballpark, was that the IFRs they assumed were far too high. The difference between an IFR of 0.8 to 0.9 percent and an IFR of 0.2 to 0.3 percent, even in the completely unrealistic worst-case scenarios, is the difference between millions and hundreds of thousands of deaths—still a grim outcome, but not nearly as bad as the horrifying projections cited by politicians to justify the sweeping restrictions they imposed.
“The parameter values in each scenario will be updated and augmented over time, as we learn more about the epidemiology of COVID-19,” the CDC cautions. “New data on COVID-19 is available daily; information about its biological and epidemiological characteristics remain[s] limited, and uncertainty remains around nearly all parameter values.” But the CDC’s current best estimates are surely better grounded than the numbers it was using two months ago.
A recent review of 13 studies that calculated IFRs in various countries found a wide range of estimates, from 0.05 percent in Iceland to 1.3 percent in Northern Italy and among the passengers and crew of the Diamond Princess cruise ship. This month Stanford epidemiologist John Ioannidis, who has long been skeptical of high IFR estimates for COVID-19, looked specifically at published studies that sought to estimate the prevalence of infection by testing people for antibodies to the virus that causes the disease. He found that the IFRs implied by 12 studies ranged from 0.02 percent to 0.4 percent. My colleague Ron Bailey last week noted several recent antibody studies that implied considerably higher IFRs, ranging from 0.6 percent in Norway to more than 1 percent in Spain.
Methodological issues, including sample bias and the accuracy of the antibody tests, probably explain some of this variation. But it is also likely that actual IFRs vary from one place to another, both internationally and within countries. “It should be appreciated that IFR is not a fixed physical constant,” Ioannidis writes, “and it can vary substantially across locations, depending on the population structure, the case-mix of infected and deceased individuals and other, local factors.”
[….]
If you focus on hard-hit areas such as New York and New Jersey, an IFR between 0.2 and 0.3 percent, as suggested by the CDC’s current best estimate, seems improbably low. “While most of these numbers are reasonable, the mortality rates shade far too low,” University of Washington biologist Carl Bergstrom told CNN. “Estimates of the numbers infected in places like NYC are way out of line with these estimates.”
But the CDC’s estimate looks more reasonable when compared to the results of antibody studies in Miami-Dade County, Santa Clara County, Los Angeles County, and Boise, Idaho—places that so far have had markedly different experiences with COVID-19. We need to consider the likelihood that these divergent results reflect not just methodological issues but actual differences in the epidemic’s impact—differences that can help inform the policies for dealing with it.
IMMUNITIES
Of course there is another twist in the whole story morning glory… even with the vaccine, the virus itself is disappearing naturally as more and more people are naturally getting immune to it through contact (most react with no or minor symptoms), the vaccine will be useless by the time it is produced. (Which is why they will in the end FORCE this on us, to vindicate the monies spent and a need to recoup costs.)
Coronavirus ‘disappearing’ so fast Oxford vaccine has ‘only 50% chance of working’ https://t.co/xui1D4MpPL
— Daniel Horowitz (@RMConservative) May 24, 2020
This is because the HERD IMMUNITY rate may be much lower that some have been saying:
Why Herd Immunity To Covid-19 Is Reached Much Earlier Than Thought (JUDITH CURRY)
… In my view, the true herd immunity threshold probably lies somewhere between the 7% and 24% implied by the cases illustrated in Figures 4 and 5. If it were around 17%, which evidence from Stockholm County suggests the resulting fatalities from infections prior to the HIT being reached should be a very low proportion of the population. The Stockholm infection fatality rate appears to be approximately 0.4%,[20] considerably lower than per the Verity et al.[21] estimates used in Ferguson20, with a fatality rate of under 0.1% from infections until the HIT was reached. The fatality rate to reach the HIT in less densely populated areas should be lower, because R0 is positively related to population density.[22] Accordingly, total fatalities should be well under 0.1% of the population by the time herd immunity is achieved. Although there would be subsequent further fatalities, as the epidemic shrinks it should be increasingly practicable to hasten its end by using testing and contact tracing to prevent infections spreading, and thus substantially reduce the number of further fatalities below those projected by the SEIR model in a totally unmitigated scenario.
Herd Immunity May Only Need 10-20 Per Cent Of People To Be Infected (SPECTATOR UK)
…The usual health warnings apply. Gomes’ work is theoretical modelling and, in common with a lot of material on Covid-19 that is being pre-published at the moment (including Ferguson’s paper of 16 March), it has not been peer-reviewed. But it is interesting that it gives an estimate for herd immunity of between 10 and 20 per cent, because that echoes real-life experience. The closest we have to a controlled experiment on the spread of Covid-19 was the cruise ship Diamond Princess, where the disease was able to spread uncontrolled in January, and almost all were later tested for the disease. Out of the 3,711 passengers and crew, 712 – or 19 per cent – were infected.
If herd immunity really is achieved at between 10 to 20 per cent it could mean that many parts of the world are approaching it – or are there already. A study of 1,000 residents in the North West German town of Gangelt in early April suggested that 14 per cent had already been infected (many without even knowing it). A study of 1,300 New Yorkers in late April suggested that 21 per cent have been infected.
Some other posts of mine noting herd immunity:
- Woodstock Occurred in the Middle of a Pandemic
- Infectious Thoughts On “The RONA” (My Facebook Posts)
% Asymptomatic Expressions %
* I also believe the CDC to be waay off in their assessment of the asymptomatic expressions of this virus. They say it is 35%, I say this is way too low. I would posit the lowest is 50%, whereas the highest is between 80% and 86%. My guess is closer to 80%. Here are some examples to support my statements:
[/color-box]When an outbreak of coronavirus in a Boston homeless shelter prompted officials to do more testing, the results caught them off guard. Of the 146 people who tested positive, all of them were considered asymptomatic.
“These are larger numbers than we ever anticipated,” said Dr. Jim O’Connell, president of the Boston Health Care for the Homeless Program. “Asymptomatic spread is something we’ve underestimated overall, and it’s going to make a big difference.”…
(CNN)
…Dr. Michael Para with OSU said the mass testing was a critical step.
“A large number were positive, but what is amazing is how many people were positive and had no symptoms at all. They were feeling fine,” he said.
Mass testing at the Marion Correctional Institution, for example, revealed that approximately 96 percent of inmates who tested positive for COVID-19 were asymptomatic, Chambers-Smith added.
Para said clinicians looked at what they had found and they are now testing the people who were negative to see if they have turned positive.
“Going forward we are going to test specific individuals who are showing symptoms, who are being released, etc.,” he said. “By testing inmates on release, we can notify local health departments whether or not a person is COVID-19 positive.”…
(FOX19)
MORE
[1] “There are probably 25 to 50 people who have the virus for every one person who is confirmed” — Dr. Marty Makary
Here is my uploaded (truncated) video of Dr. Makary (John Hopkins) being interviewed by YAHOO FINANCE (see their FULL video at YouTube HERE):
[2] 86% of infections went undocumented — Science Journal
Here, the NEW YORK POST (March 17, 2020) notes the journal article by saying:
“Stealth” coronavirus cases are fueling the pandemic, with a staggering 86% of people infected walking around undetected, a new study says.
Six of every seven cases – 86% — were not reported in China before travel restrictions were implemented, driving the spread of the virus, according to a study Monday in the journal Science.
“It’s the undocumented infections which are driving the spread of the outbreak,” said co-author Jeffrey Shaman of Columbia University Mailman School, according to GeekWire.
Using computer modeling, researchers tracked infections before and after the Chinese city of Wuhan’s travel ban.
The findings indicated that these undocumented infections with no or mild symptoms — known as “stealth” cases — were behind two-thirds of the reported patients.
“The majority of these infections are mild, with few symptoms at all,” Shaman said, Mercury News reported. “People may not recognize it. Or they think they have a cold.”…
This information likewise calls into question the “official numbers of deaths” being attributed to the CDC as well as supporting the idea that many more persons have the WU FLU, making the death rate percentages even smaller than being discussed above. I am repeating the below because I think it is crucially important!
Enjoy:
other PERTINENT information
MAY I ALSO NOTE that I believe the deaths from The Rona are a bit overstated, while Dr. Birx noted that the CDC may be inflating the death toll by 25%, I provide a couple other examples to support my claim.
UPDATED INFO – Real Quick
![]() On Thursday, the Washington State Department of Health (DOH) confirmed a report by the Freedom Foundation that they have included those who tested positive for COVID-19 but died of other causes, including gunshot injuries, in their coronavirus death totals. This calls into serious question the state’s calculations of residents who have actually died of the CCP pandemic.
On Thursday, the Washington State Department of Health (DOH) confirmed a report by the Freedom Foundation that they have included those who tested positive for COVID-19 but died of other causes, including gunshot injuries, in their coronavirus death totals. This calls into serious question the state’s calculations of residents who have actually died of the CCP pandemic.
(PJ-MEDIA)
First up, Dr. Birx setting the stage for this with how deaths are coded:
Another example comes from Dr. Ngozi, Director of public health Illinois. She explains how ALL deaths are counted as Covid-19 even if the patient was diagnosed to have die from another disease:
Adapted from the above video description is important (via 4 TIMES A YEAR)
“Should “COVID-19” be reported on the death certificate only with a confirmed test? COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death.” (CDC): “Deborah Birx, a physician who’s leading the White House’s coronavirus task force, said Alabama’s strategy conflicts with CDC’s approach to tallying Covid-19-realted deaths. “[W]e’ve taken a very liberal approach to mortality,” she said. “[I]f someone dies with Covid-19, we are counting that as a Covid-19 death.” (ADVISORY)
As many have pointed out, there is a big difference between dying WITH the virus and FROM the virus.
Note Dr. Birx’s similar wording to what Italy was doing:
“‘We’ve taken a very liberal approach to mortality….” “The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus.”
Italy, unlike the CDC, corrected its error:
“The age of our patients in hospitals is substantially older – the median is 67, while in China it was 46,” Prof Ricciardi says. “So essentially the age distribution of our patients is squeezed to an older age and this is substantial in increasing the lethality.”
A study in JAMA this week found that almost 40 per cent of infections and 87 per cent of deaths in the country have been in patients over 70 years old.
[….]
But Prof Ricciardi added that Italy’s death rate may also appear high because of how doctors record fatalities.
“The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus.
“On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus, while 88 per cent of patients who have died have at least one pre-morbidity – many had two or three,” he says.
[….]
If further testing finds more asymptomatic cases spreading undetected, the mortality rate will drop.
Here is more information from Daniel Horowitz over at CONSERVATIVE REVIEW:
1) The shocking inflation of COVID-19 death numbers: From day one, we were warned that states are ascribing every single death of anyone who happens to test positive for the coronavirus — even if they are asymptomatic — to the virus rather than the clear cause of death. Now, thanks to a lawsuit in Colorado, the state was forced to revise its death count down by 23 % over the weekend — from 1,150 to 878. The state is now publishing numbers of deaths “with” COVID-19 separate from deaths “from” COVID-19. As I reported on Thursday, county officials started accusing the state’s department of health of reclassifying deaths of those who tested positive for the virus but died of things like alcohol poisoning as COVID-19 deaths just to insidiously inflate the numbers. This revision in Colorado is a bombshell story that, of course, will remain unknown to most Americans. Every state needs to do this, and if they did, we would find an across-the-board drop in numbers by at least 25%, the same %age by which Dr. Birx reportedly believes the count is being inflated, according to the Washington Post. For example, in Minnesota, state officials are now admitting that every single person who dies in a nursing home after testing positive is now deemed to have died from the virus, never mind the fact that 25% of all natural deaths in a given week occur in nursing homes and that most cases of COVID-19 are asymptomatic, which means more often than not, they died exclusively of other causes.
TO WIT… Dennis Prager’s guest is Dr. Joel Hay, who is a professor in the department of Pharmaceutical Economics and Policy at the University of Southern California. Both give examples of cancer deaths being coded Covid:
And my third evidence to support my contention a nurse is filmed commenting on the percentages of deaths at NYC hospital. In my posts point #2 (the video still up amazingly) notes that every death cert in NYC-hospital is coded as Rona. In fact, 99% of deaths from that hospital were coded Rona during a period — AN IMPOSSIBLE statistic (https://tinyurl.com/y9awsuor — my site)
A CLEARER PICTURE blog comments on the above indirectly:
….In New York City, around 12,000 people have supposedly died from COVID-19 at the time of this writing. That’s 22% of all alleged U.S. deaths.
Around 7,000 of the NYC deaths attributed to COVID-19 have been thoroughly investigated to determine if there was another serious life-threatening illness present
Take a deep breath if doing so hasn’t been outlawed where you live.
99.2% of those 7,000 New Yorkers who supposedly died from the virus had another antecedent life-threatening illness. For all intents and purposes, that’s all of them.
How is it even remotely possible that 7,000 NYC deaths attributed to COVID-19 were investigated and virtually every single one of them found to have involved at least one other life-threatening illness if the virus is in and of itself deadly?
Most strains of coronavirus that affect humans are common cold viruses.
In light of the apparent almost universal prevalence of at least one other deadly disease among the alleged NYC deceased…
And in light of all the factors massively inflating the bogus death tally we’re being fed every day…
What reason do we have to believe COVID-19 is actually killing anyone?
No one knows how many Americans have really died of COVID-19….
However, we are starting to find out that “pure” deaths caused by Covid-19 exclusivelt is low (DAILY WIRE):
On Tuesday, San Diego county Supervisor Jim Desmond said after digging into the data that he believes only six of the county’s 194 coronavirus-identified deaths are “pure” coronavirus deaths, meaning they died from the virus, not merely with the virus.
Desmond was seemingly ruling out deaths from individuals with preexisting conditions.
“We’ve unfortunately had six pure, solely coronavirus deaths — six out of 3.3 million people,” Desmond said on a podcast, Armstrong & Getty Extra Large Interviews, according to San Diego Tribune. “I mean, what number are we trying to get to with those odds. I mean, it’s incredible. We want to be safe, and we can do it, but unfortunately, it’s more about control than getting the economy going again and keeping people safe.”
Public Health Officer Dr. Wilma Wooten suggested Wednesday during a press briefing that Desmond was being callous, noting that their liberal identification of COVID-19 deaths is uniform with coding nationwide.
“Their life is no less valuable than someone’s life who does not have underlying medical conditions,” Wooten said. “This is not just San Diego. This is how this is done throughout the entire nation in terms of identifying who has died of COVID-19.”…
Also note that all the anti-body tests are showing a larger infected population than previously considered. REASON.COM previously noted the Stanford study that between “48,000 and 81,000 residents of Santa Clara County, California are likely to have already been infected by the coronavirus that causes COVID-19.” Stanford University has revised the numbers to better fit the assumption (via MERCURY NEWS):
…In a revised analysis of a startling study published last month, they now estimate that 2.8% of Santa Clara residents were previously infected by the virus but didn’t know it.
That implies that the county had up to 54,000 infections — many more than the 1,000 confirmed cases in the county at the time.
“This suggests that the large majority of the population does not have antibodies and may be susceptible to the virus,” concludes the research paper, published in the online report medRxiv….
MY COMMENTS FROM MY FACEBOOK ABOUT THE ABOVE
So, Stanford settled on a number in early April… when there were 1,000 CONFIRMED cases were known in Santa Clara, there were 54,000 infected. To REALLY understand the percentages you would have to follow those 1,000 KNOWN cases from that time and compare the 55,000 cases to those deaths. (BTW, Stanford took the lower path on stats; so there could be a larger number.) Here is part of the article… but know that with the flu shot, there are more deaths by the flu than The Rona, without a “Rona shot.”
UPDATE (trying to figure out deaths per infections): Okay, let us apply the 98% survive who are known to have it and are hospitalized stat I have heard for some time. So 2% of the 1,000 is 20. 20 deaths from that early April figure of 55,000. Right? Gives you… 0.036%
UPDATES!
A friend on FACEBOOK has been a light in the war-torn field of The Rona (Wu Flu) battle of infection rates. Here are two posts of his [combined with a response to a friendly comment from one of his peeps] followed by some recent articles (links to papers will be in graphics):
Here’s a new meta-study from Stanford of all of the antibody testing that’s happened.
This puts the Wu Flu anywhere between 7x LESS deadly than the flu and 2.8x MORE deadly than the flu (making it a little worse than a bad flu season like 2018). And that’s assuming that this doesn’t follow SARS 1 and just disappear.
The data behind this is really solid, and the author is well-respected. Unlike those stupid models we were using, this is really real data.
We don’t do contact tracing, social distancing, mask-wearing, or lockdowns for the seasonal flu, and this looks like a watered down seasonal flu that got 100000000x more media attention and governors sending sick people to nursing homes to boost up the death rate.
The original post (OP) on this second strain was a graphic. I will link to the Kent County (Michigan site through it. Here is my FB description of the following: “A person named B.M. wrote on a friends Facebook wall the following regarding “contact tracing.” (The original post had to do with hiring government employees to trace citizens with Covid.)”
(See also this BRIDGE article)
- [A reader of JP’s noted] Actually, contact tracing sounds like a legitimate work of government. Rather than quarantining the healthy, quarantine the sick and monitor those exposed to the disease.
JP responded:
Sorry in advance for the novel! Heh, I started thinking of other interesting things to add and just decided to run with it.
Contact tracing might work for illnesses that don’t spread very easily (it probably would have exterminated HIV, according to what I’ve read; I’m no expert but it seems reasonable), but for upper respiratory stuff like colds and flus (and the Wu Flu), it’s pretty much doomed, especially with up to 10% of the whole country already having the it.
The original point of the lockdowns (which don’t seem to have worked; lockdown and non-lockdown countries and states have almost identical statistics) was to slow the spread to prevent hospitals from being overwhelmed. It wasn’t to stop spread, since even the CDC admits that after about 1% of people are infected with a contagious disease, you can’t really close the door on it anymore. Contact tracing is a relatively invasive way of closing the door on a virus, so I don’t think it will work here**.
The data points to a much less lethal bug, though. Stanford’s meta analysis of all of the large-scale antibody testing shows an IFR (Infection Fatality Rate) between 7 times less than the seasonal flu and 2.8 times more. It’s probably in the middle, making it slightly less lethal than regular seasonal flus. And since we know it has been in the US at least since January (probably since December or earlier), the R? (Basic Reproduction Number or Rate) is also much lower than people originally thought. So it spreads like the flu and is as deadly as the flu.
The main difference seems to be the 24/7 media terrorizing of citizens, the complete ignorance most of us (that’s me, too) had in the real pneumonia/influenza deaths each year, and the downright evil policy of many Democrat governors of sending the sick to recover (while contagious) at nursing homes, boosting the deaths by up to 50%.
Sorry for the novel!! Reading every little bit about this thing has become an unfortunate hobby of mine. I’m of the mind now that the best strategy is to fight the fear instead of the virus and to get back to normal in virtually every way. If this is anything like it’s older brother SARS, it will die out in the next couple of months. But if not, keeping everyone from immunity just means extending the risk.
** I think contact tracing may -appear- to work because I think we are naturally bottoming out cases. Same, in my mind, for other measures.
One final bit: I’ve followed lots of different predictions to see who might get things most accurately to see what they did differently. This guy’s been right on (it’s been almost scary) using SARS as a comparison instead of the Spanish Flu (since this bug is SARS 2). This is a really good visual of the whole thing:
(Click to enlarge)

ALSO, a short bit from Bruce Carrol:
“If you are waiting for a “cure” for COVID-19, you’ll never leave your home again.
Even the flu vaccine (not vaccine, flu shot. There is a vaccine for the Polio, not HIV or SARS) results in 60-80,000 deaths every season.
We have to stop the fearmongering and start learning to live with a new virus in a string of new viruses that have emerged for tens of thousands of years.
Boomers and Millennials aren’t that special of a species.”
— Bruce Carroll (Co-founder of the gay Republican group GOProu, and founder of GAYPATRIOT)
The SPECTATOR USA has an excellent article backing up the above conversation, entitled, “Stanford Study Suggests Coronavirus Might Not Be As Deadly As Flu: All their estimates for IFR are markedly lower than the figures thrown about a couple of months ago” (This was a SPECTATOR UK original piece – FYI)
One of the great unknowns of the COVID-19 crisis is just how deadly the disease is. Much of the panic dates from the moment, in early March, when the World Health Organization (WHO) published a mortality rate of 3.2 percent — which turned out to be a crude ‘case fatality rate’ dividing the number of deaths by the number of recorded cases, ignoring the large number of cases which are asymptomatic or otherwise go unrecorded.
The Imperial College modeling, which has been so influential on the UK government, assumed an infection fatality rate (IFR) of 0.9 percent. This was used to compute the infamous prediction that 250,000 Britons would die unless the government abandoned its mitigation strategy and adopted instead a policy of suppressing the virus through lockdown. Imperial later revised its estimate of the IFR down to 0.66 percent — although the March 16 paper which predicted 250,000 deaths was not updated.
In the past few weeks, a slew of serological studies estimating the prevalence of infection in the general population has become available. This has allowed Prof John Ioannidis of Stanford University to work out the IFR in 12 different locations.
They range between 0.02 percent and 0.5 percent — although Ioannidis has corrected those raw figures to take account of demographic balance and come up with estimates between 0.02 percent and 0.4 percent. The lowest estimates came from Kobe, Japan, found to have an IFR of 0.02 percent and Oise in northern France, with an IFR of 0.04 percent. The highest were in Geneva (a raw figure of 0.5 percent) and Gangelt in Germany (0.28 percent).
The usual caveats apply: most studies to detect the prevalence of the SARS-CoV-2 virus in the general population remain unpublished, and have not yet been peer-reviewed. Some are likely to be unrepresentative of the general population. The Oise study, in particular, was based on students, teachers and parents in a single high school which was known to be a hotspot on COVID-19 infection. At the other end of the table, Geneva has a relatively high age profile, which is likely to skew its death rate upwards.
But it is noticeable how all these estimates for IFR are markedly lower than the figures thrown about a couple of months ago, when it was widely asserted that COVID-19 was a whole magnitude worse than flu. Seasonal influenza is often quoted as having an IFR of 0.1 to 0.2 percent. The Stanford study suggests that COVID-19 might not, after all, be more deadly than flu — although, as Ioannidis notes, the profile is very different: seasonal flu has a higher IFR in developing countries, where vaccination is rare, while COVID-19 has a higher death rate in the developed world, thanks in part of more elderly populations.
The Stanford study, however, does not include the largest antibody study to date: that involving a randomized sample of 70,000 Spanish residents, whose preliminary results were published by the Carlos III Institute of Health two weeks ago. That suggested that five percent of the Spanish population had been infected with the virus. With 27,000 deaths in the country, that would convert to an IFR of 1.1 percent.
This backs up of course some excellent article by Daniel Horowitz:
- One Chart Exposes The Lie Behind Universal Lockdowns
- Ep 641 | Everything You Need to Know About Antibody Tests
- Lockdowns Missed The Boat: More Likely Coronavirus Cases In Us As Early As December
- We Have Been Lied To: 6 Facts That Change Everything We Know About SARS-CoV-2
A CLEARER PICTURE has a great post about this as well, I suggest if you like what you see you check out that blog weekly.
…For one thing, Dr. Fauci and Dr. Birx have both explicitly stated that anyone dying WITH the virus is counted as dying FROM it. Since 4/5 of COVID-19 infections are mild and 1/2 appear to show no symptoms at all, the official U.S. death tally is bound to include many in which it played little or no role.
The CDC has made matters much worse by insisting that doctors list COVID-19 on death certificates without a positive test confirming its presence and even absent any medical justification at all. A willingness to “assume” it was a factor is all that’s officially required. And hospitals now reap enormous financial rewards for making the assumption.
(Click To Enlarge)
![]()
Those in charge couldn’t have possibly shown less interest in determining the real number of Americans who would still be alive if not for having contracted COVID-19. It’s unlikely that ours is the only country in which the data has been turned into garbage by a perfect storm of inflating factors. As hard as it may be to accept, the odds are pretty much nil that we’ll ever know how deadly the virus we were made to spend months obsessively fearing really was.
Even on the inflated numbers we’re getting, however, it isn’t anywhere near 10 times deadlier than the flu; as Dr. Fauci claimed on March 11, while ginning up support for his novel public health strategy of extinguishing our rights and wrecking the economy. But, of course, a few weeks later, we learned that even Fauci didn’t believe a word of the lie he so effectively used to terrorize a nation of over 300 million people into suicidal obedience.
Though perhaps you haven’t heard. You see, on March 26, Dr. Fauci shared his true opinion with his peers in the pages of the prestigious New England Journal of Medicine:
The overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%).
Dr. Anthony Fauci, March 26, 2020 New England Journal of Medicine
In case you’re wondering, the parenthetical remark is his, not mine. Moreover, when Sharyl Attkisson contacted the journal about the strange discrepancy between what Fauci was scaring the public with and the substantially less alarming take his learned colleagues heard, she discovered his article had been submitted “many weeks ago.”….

