JUMP TO…
- Ages of deaths for getting Covid-19[84]
- A Blue State Disease
- A Fatal Andrew Cuomo Call
- Too Many Deaths Said To Be Covid-19[84]
- UPDATES
More than half of U.S. deaths are from nursing homes — THE GUARDIAN:
- Yale professor describes as ‘staggering’ research that reveals more than half of all deaths in 14 US states from elderly care facilities
The average age group who dies from “The Rona” is found here in the latest from WORLD O’METER:
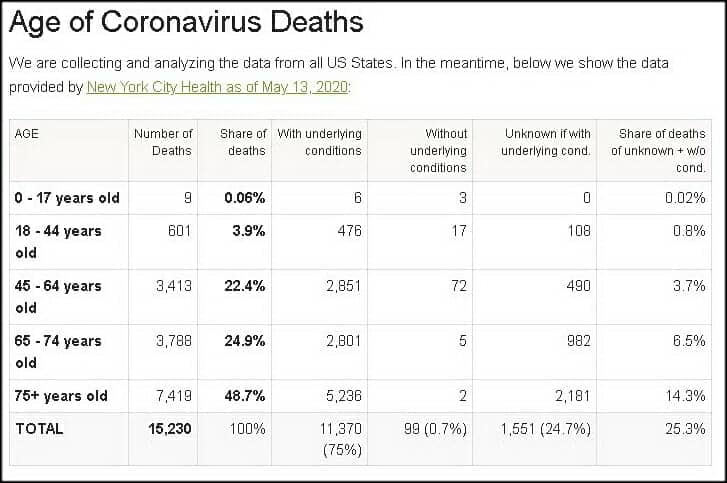
Not only that, but the co-morbidities (just as in flu deaths) are high and in multiples. Some examples:
- Of the 22,332 people who died in hospital in England between 31 March and 12 May, 5,873 (26%) suffered from either type 1 or type 2 diabetes, NHS England figures reveal. That was the most common illness found in an analysis of what existing conditions patients had. The other commonest comorbidities were dementia (18%), serious breathing problems (15%) and chronic kidney disease (14%). One in ten (10%) suffered from ischaemic heart disease. (GUARDIAN)
- A new study published April 22 in the Journal of the American Medical Association characterizes the symptoms, comorbidities, and clinical outcomes of 5,700 patients hospitalized because of COVID-19 in the New York area. The authors found that 94 percent of the patients had a chronic health problem, and 88 percent had two or more. The three most prevalent conditions were hypertension (56.6 percent), obesity (41.7 percent), and diabetes (33.8 percent). (THE SCIENTIST)
Now, many of these deaths were preventable, but for some reason many of the hardest hit states had a tragic policy of sending elderly patients back to nursing homes to recover. Many of the blue states, where most of the deaths have occurred:
- If you live in New Jersey, you are 13 times more likely to die from COVID-19 than if you live in Florida. The Garden State’s death rate per million is 895.2, according to the RealClearPolitics coronavirus tracker, compared to only 65.1 deaths per million for Florida. This disparity can’t be written off to demography or testing. Florida has a huge elderly population, and it has conducted twice as many tests as New Jersey. (AMERICAN SPECTATOR)

I have a slew of articles regarding this deadly choice by Andrew Cuomo on my site (FULLY reproduced here):
Governor Andrew Cuomo’s Deadly Decision
ERIC METAXAS interviews John Zmirak about his article, “Why Is Andrew Cuomo Killing Patients In Nursing Homes? Imagine If We’D Responded To AIDS By Closing Everything BUT The Gay Bath Houses” (THE STREAM), that puts Governor Cuomo’s “fatal decision” regarding Covid-19 and nursing homes squarely in the bullseye.
Here are SOME of the other stories (earliest to latest) you have probably not heard reported about in the MSM:
- Andrew Cuomo’s Coronavirus Nursing Home Policy Proves Tragic (NEW YORK POST);
- Gov. Cuomo Says ‘It’s Not Our Job’ To Provide PPE To Nursing Homes (NEW YORK POST);
- Forcing Nursing Homes To Take Coronavirus Patients Is Just Insane — And Evil (NEW YORK POST);
- State Lacked Common Sense In Nursing Homes Coronavirus Approach (NEW YORK POST);
- Cuomo Doubles Down On Ordering Nursing Homes To Admit Coronavirus Patients (NEW YORK POST);
- Andrew Cuomo Under Fire for Directive Requiring Nursing Homes to Accept Coronavirus Patients (BREITBART);
- New York Required Nursing Homes To Admit ‘Medically Stable’ Coronavirus Patients. The Results Were Deadly (DAILY WIRE)
- ‘Blood On His Hands’: Mark Levin Rips Andrew Cuomo Over ‘Deadly Fiat’ Nursing Home Controversy (WASHINGTON EXAMINER);
- Three Hardest-Hit, Democrat-Run States Force Nursing Homes To Accept Recovering COVID Patients, Face Backlash (DAILY WIRE);
- Cuomo Claims He Didn’t Know About New York Rule Forcing Nursing Homes To Accept Elderly With COVID-19 (THE FEDERALIST);
- Cuomo To Blame For Covid Spreading Through Nursing Home (NEW YORK POST);
- Media Doesn’t Care That People Died Because Cuomo Put Coronavirus Patients In Nursing Homes (THE FEDERALIST).
I have some older posts dealing with [in some way] Andrew Cuomo (Apparently I only post about Governor Cuomo in the first half of the year?):
- The Housing Crisis of 2008 Revisited – April 14, 2020
- A Real Border Crisis (Not Manufactured) – April 3, 2019
- White Castle vs. New York Values – April 19, 2016
- Leftist Ideals Exemplified ~ Cuba vs. North Carolina – March 30, 2016
- Glenn Beck Blasts Cuomo`s Remark Against Conservatives (Reflections of Fox Included) – January 22, 2014
End of Reproduction
MAY I ALSO NOTE that I believe the deaths from The Rona are a bit overstated, while Dr. Birx noted that the CDC may be inflating the death toll by 25%, I provide a couple other examples to support my claim. First up, Dr. Birx setting the stage for this with how deaths are coded:
Another example comes from Dr. Ngozi, Director of public health Illinois. She explains how ALL deaths are counted as Covid-19 even if the patient was diagnosed to have die from another disease:
Here is more information from Daniel Horowitz over at CONSERVATIVE REVIEW:
1) The shocking inflation of COVID-19 death numbers: From day one, we were warned that states are ascribing every single death of anyone who happens to test positive for the coronavirus — even if they are asymptomatic — to the virus rather than the clear cause of death. Now, thanks to a lawsuit in Colorado, the state was forced to revise its death count down by 23 % over the weekend — from 1,150 to 878. The state is now publishing numbers of deaths “with” COVID-19 separate from deaths “from” COVID-19. As I reported on Thursday, county officials started accusing the state’s department of health of reclassifying deaths of those who tested positive for the virus but died of things like alcohol poisoning as COVID-19 deaths just to insidiously inflate the numbers. This revision in Colorado is a bombshell story that, of course, will remain unknown to most Americans. Every state needs to do this, and if they did, we would find an across-the-board drop in numbers by at least 25%, the same %age by which Dr. Birx reportedly believes the count is being inflated, according to the Washington Post. For example, in Minnesota, state officials are now admitting that every single person who dies in a nursing home after testing positive is now deemed to have died from the virus, never mind the fact that 25% of all natural deaths in a given week occur in nursing homes and that most cases of COVID-19 are asymptomatic, which means more often than not, they died exclusively of other causes.
TO WIT… Dennis Prager’s guest is Dr. Joel Hay, who is a professor in the department of Pharmaceutical Economics and Policy at the University of Southern California. Both give examples of cancer deaths being coded Covid:
And my third evidence to support my contention a nurse is filmed commenting on the percentages of deaths at NYC hospital. In my posts point #2 (the video still up amazingly) notes that every death cert in NYC-hospital is coded as Rona. In fact, 99% of deaths from that hospital were coded Rona during a period — AN IMPOSSIBLE statistic (https://tinyurl.com/y9awsuor — my site)
A CLEARER PICTURE blog comments on the above indirectly:
….In New York City, around 12,000 people have supposedly died from COVID-19 at the time of this writing. That’s 22% of all alleged U.S. deaths.
Around 7,000 of the NYC deaths attributed to COVID-19 have been thoroughly investigated to determine if there was another serious life-threatening illness present
Take a deep breath if doing so hasn’t been outlawed where you live.
99.2% of those 7,000 New Yorkers who supposedly died from the virus had another antecedent life-threatening illness. For all intents and purposes, that’s all of them.
How is it even remotely possible that 7,000 NYC deaths attributed to COVID-19 were investigated and virtually every single one of them found to have involved at least one other life-threatening illness if the virus is in and of itself deadly?
Most strains of coronavirus that affect humans are common cold viruses.
In light of the apparent almost universal prevalence of at least one other deadly disease among the alleged NYC deceased…
And in light of all the factors massively inflating the bogus death tally we’re being fed every day…
What reason do we have to believe COVID-19 is actually killing anyone?
No one knows how many Americans have really died of COVID-19….
However, we are starting to find out that “pure” deaths caused by Covid-19 exclusivelt is low (DAILY WIRE):
On Tuesday, San Diego county Supervisor Jim Desmond said after digging into the data that he believes only six of the county’s 194 coronavirus-identified deaths are “pure” coronavirus deaths, meaning they died from the virus, not merely with the virus.
Desmond was seemingly ruling out deaths from individuals with preexisting conditions.
“We’ve unfortunately had six pure, solely coronavirus deaths — six out of 3.3 million people,” Desmond said on a podcast, Armstrong & Getty Extra Large Interviews, according to San Diego Tribune. “I mean, what number are we trying to get to with those odds. I mean, it’s incredible. We want to be safe, and we can do it, but unfortunately, it’s more about control than getting the economy going again and keeping people safe.”
Public Health Officer Dr. Wilma Wooten suggested Wednesday during a press briefing that Desmond was being callous, noting that their liberal identification of COVID-19 deaths is uniform with coding nationwide.
“Their life is no less valuable than someone’s life who does not have underlying medical conditions,” Wooten said. “This is not just San Diego. This is how this is done throughout the entire nation in terms of identifying who has died of COVID-19.”…
Also note that all the anti-body tests are showing a larger infected population than previously considered. REASON.COM previously noted the Stanford study that between “48,000 and 81,000 residents of Santa Clara County, California are likely to have already been infected by the coronavirus that causes COVID-19.” Stanford University has revised the numbers to better fit the assumption (via MERCURY NEWS):
…In a revised analysis of a startling study published last month, they now estimate that 2.8% of Santa Clara residents were previously infected by the virus but didn’t know it.
That implies that the county had up to 54,000 infections — many more than the 1,000 confirmed cases in the county at the time.
“This suggests that the large majority of the population does not have antibodies and may be susceptible to the virus,” concludes the research paper, published in the online report medRxiv….
MY COMMENTS FROM MY FACEBOOK ABOUT THE ABOVE
So, Stanford settled on a number in early April… when there were 1,000 CONFIRMED cases were known in Santa Clara, there were 54,000 infected. To REALLY understand the percentages you would have to follow those 1,000 KNOWN cases from that time and compare the 55,000 cases to those deaths. (BTW, Stanford took the lower path on stats; so there could be a larger number.) Here is part of the article… but know that with the flu shot, there are more deaths by the flu than The Rona, without a “Rona shot.”
UPDATE (trying to figure out deaths per infections): Okay, let us apply the 98% survive who are known to have it and are hospitalized stat I have heard for some time. So 2% of the 1,000 is 20. 20 deaths from that early April figure of 55,000. Right? Gives you… 0.036%
UPDATES!
A friend on FACEBOOK has been a light in the war-torn field of The Rona (Wu Flu) battle of infection rates. Here are two posts of his [combined with a response to a friendly comment from one of his peeps] followed by some recent articles (links to papers will be in graphics):
Here’s a new meta-study from Stanford of all of the antibody testing that’s happened.
This puts the Wu Flu anywhere between 7x LESS deadly than the flu and 2.8x MORE deadly than the flu (making it a little worse than a bad flu season like 2018). And that’s assuming that this doesn’t follow SARS 1 and just disappear.
The data behind this is really solid, and the author is well-respected. Unlike those stupid models we were using, this is really real data.
We don’t do contact tracing, social distancing, mask-wearing, or lockdowns for the seasonal flu, and this looks like a watered down seasonal flu that got 100000000x more media attention and governors sending sick people to nursing homes to boost up the death rate.
The original post (OP) on this second strain was a graphic. I will link to the Kent County (Michigan site through it. Here is my FB description of the following: “A person named B.M. wrote on a friends Facebook wall the following regarding “contact tracing.” (The original post had to do with hiring government employees to trace citizens with Covid.)”
(See also this BRIDGE article)
- [A reader of JP’s noted] Actually, contact tracing sounds like a legitimate work of government. Rather than quarantining the healthy, quarantine the sick and monitor those exposed to the disease.
JP responded:
Sorry in advance for the novel! Heh, I started thinking of other interesting things to add and just decided to run with it.
Contact tracing might work for illnesses that don’t spread very easily (it probably would have exterminated HIV, according to what I’ve read; I’m no expert but it seems reasonable), but for upper respiratory stuff like colds and flus (and the Wu Flu), it’s pretty much doomed, especially with up to 10% of the whole country already having the it.
The original point of the lockdowns (which don’t seem to have worked; lockdown and non-lockdown countries and states have almost identical statistics) was to slow the spread to prevent hospitals from being overwhelmed. It wasn’t to stop spread, since even the CDC admits that after about 1% of people are infected with a contagious disease, you can’t really close the door on it anymore. Contact tracing is a relatively invasive way of closing the door on a virus, so I don’t think it will work here**.
The data points to a much less lethal bug, though. Stanford’s meta analysis of all of the large-scale antibody testing shows an IFR (Infection Fatality Rate) between 7 times less than the seasonal flu and 2.8 times more. It’s probably in the middle, making it slightly less lethal than regular seasonal flus. And since we know it has been in the US at least since January (probably since December or earlier), the R? (Basic Reproduction Number or Rate) is also much lower than people originally thought. So it spreads like the flu and is as deadly as the flu.
The main difference seems to be the 24/7 media terrorizing of citizens, the complete ignorance most of us (that’s me, too) had in the real pneumonia/influenza deaths each year, and the downright evil policy of many Democrat governors of sending the sick to recover (while contagious) at nursing homes, boosting the deaths by up to 50%.
Sorry for the novel!! Reading every little bit about this thing has become an unfortunate hobby of mine. I’m of the mind now that the best strategy is to fight the fear instead of the virus and to get back to normal in virtually every way. If this is anything like it’s older brother SARS, it will die out in the next couple of months. But if not, keeping everyone from immunity just means extending the risk.
** I think contact tracing may -appear- to work because I think we are naturally bottoming out cases. Same, in my mind, for other measures.
One final bit: I’ve followed lots of different predictions to see who might get things most accurately to see what they did differently. This guy’s been right on (it’s been almost scary) using SARS as a comparison instead of the Spanish Flu (since this bug is SARS 2). This is a really good visual of the whole thing:
(Click to enlarge)

ALSO, a short bit from Bruce Carrol:
“If you are waiting for a “cure” for COVID-19, you’ll never leave your home again.
Even the flu vaccine (not vaccine, flu shot. There is a vaccine for the Polio, not HIV or SARS) results in 60-80,000 deaths every season.
We have to stop the fearmongering and start learning to live with a new virus in a string of new viruses that have emerged for tens of thousands of years.
Boomers and Millennials aren’t that special of a species.”
— Bruce Carroll (Co-founder of the gay Republican group GOProu, and founder of GAYPATRIOT)
TO WIT…
The SPECTATOR USA has an excellent article backing up the above conversation, entitled, “Stanford Study Suggests Coronavirus Might Not Be As Deadly As Flu: All their estimates for IFR are markedly lower than the figures thrown about a couple of months ago” (This was a SPECTATOR UK original piece – FYI)
One of the great unknowns of the COVID-19 crisis is just how deadly the disease is. Much of the panic dates from the moment, in early March, when the World Health Organization (WHO) published a mortality rate of 3.2 percent — which turned out to be a crude ‘case fatality rate’ dividing the number of deaths by the number of recorded cases, ignoring the large number of cases which are asymptomatic or otherwise go unrecorded.
The Imperial College modeling, which has been so influential on the UK government, assumed an infection fatality rate (IFR) of 0.9 percent. This was used to compute the infamous prediction that 250,000 Britons would die unless the government abandoned its mitigation strategy and adopted instead a policy of suppressing the virus through lockdown. Imperial later revised its estimate of the IFR down to 0.66 percent — although the March 16 paper which predicted 250,000 deaths was not updated.
In the past few weeks, a slew of serological studies estimating the prevalence of infection in the general population has become available. This has allowed Prof John Ioannidis of Stanford University to work out the IFR in 12 different locations.
They range between 0.02 percent and 0.5 percent — although Ioannidis has corrected those raw figures to take account of demographic balance and come up with estimates between 0.02 percent and 0.4 percent. The lowest estimates came from Kobe, Japan, found to have an IFR of 0.02 percent and Oise in northern France, with an IFR of 0.04 percent. The highest were in Geneva (a raw figure of 0.5 percent) and Gangelt in Germany (0.28 percent).
The usual caveats apply: most studies to detect the prevalence of the SARS-CoV-2 virus in the general population remain unpublished, and have not yet been peer-reviewed. Some are likely to be unrepresentative of the general population. The Oise study, in particular, was based on students, teachers and parents in a single high school which was known to be a hotspot on COVID-19 infection. At the other end of the table, Geneva has a relatively high age profile, which is likely to skew its death rate upwards.
But it is noticeable how all these estimates for IFR are markedly lower than the figures thrown about a couple of months ago, when it was widely asserted that COVID-19 was a whole magnitude worse than flu. Seasonal influenza is often quoted as having an IFR of 0.1 to 0.2 percent. The Stanford study suggests that COVID-19 might not, after all, be more deadly than flu — although, as Ioannidis notes, the profile is very different: seasonal flu has a higher IFR in developing countries, where vaccination is rare, while COVID-19 has a higher death rate in the developed world, thanks in part of more elderly populations.
The Stanford study, however, does not include the largest antibody study to date: that involving a randomized sample of 70,000 Spanish residents, whose preliminary results were published by the Carlos III Institute of Health two weeks ago. That suggested that five percent of the Spanish population had been infected with the virus. With 27,000 deaths in the country, that would convert to an IFR of 1.1 percent.
This backs up of course some excellent article by Daniel Horowitz:
- One Chart Exposes The Lie Behind Universal Lockdowns
- Ep 641 | Everything You Need to Know About Antibody Tests
- Lockdowns Missed The Boat: More Likely Coronavirus Cases In Us As Early As December
- We Have Been Lied To: 6 Facts That Change Everything We Know About SARS-CoV-2
A CLEARER PICTURE has a great post about this as well, I suggest if you like what you see you check out that blog weekly.
…For one thing, Dr. Fauci and Dr. Birx have both explicitly stated that anyone dying WITH the virus is counted as dying FROM it. Since 4/5 of COVID-19 infections are mild and 1/2 appear to show no symptoms at all, the official U.S. death tally is bound to include many in which it played little or no role.
The CDC has made matters much worse by insisting that doctors list COVID-19 on death certificates without a positive test confirming its presence and even absent any medical justification at all. A willingness to “assume” it was a factor is all that’s officially required. And hospitals now reap enormous financial rewards for making the assumption.
(Click To Enlarge)
![]()
Those in charge couldn’t have possibly shown less interest in determining the real number of Americans who would still be alive if not for having contracted COVID-19. It’s unlikely that ours is the only country in which the data has been turned into garbage by a perfect storm of inflating factors. As hard as it may be to accept, the odds are pretty much nil that we’ll ever know how deadly the virus we were made to spend months obsessively fearing really was.
Even on the inflated numbers we’re getting, however, it isn’t anywhere near 10 times deadlier than the flu; as Dr. Fauci claimed on March 11, while ginning up support for his novel public health strategy of extinguishing our rights and wrecking the economy. But, of course, a few weeks later, we learned that even Fauci didn’t believe a word of the lie he so effectively used to terrorize a nation of over 300 million people into suicidal obedience.
Though perhaps you haven’t heard. You see, on March 26, Dr. Fauci shared his true opinion with his peers in the pages of the prestigious New England Journal of Medicine:
The overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%).
Dr. Anthony Fauci, March 26, 2020 New England Journal of Medicine
In case you’re wondering, the parenthetical remark is his, not mine. Moreover, when Sharyl Attkisson contacted the journal about the strange discrepancy between what Fauci was scaring the public with and the substantially less alarming take his learned colleagues heard, she discovered his article had been submitted “many weeks ago.”….